A lumen-apposing metal stent (LAMS) is an innovative device recently developed for use in interventional endoscopy, with re-purposed LAMS applications constantly being introduced [1]. For an increasingly multimorbid population with complicated bile duct stone disease and rigorous indications for dual antiplatelet therapy (DAPT), implying both high procedural and thrombotic risk, endoscopic management strategies vary widely.
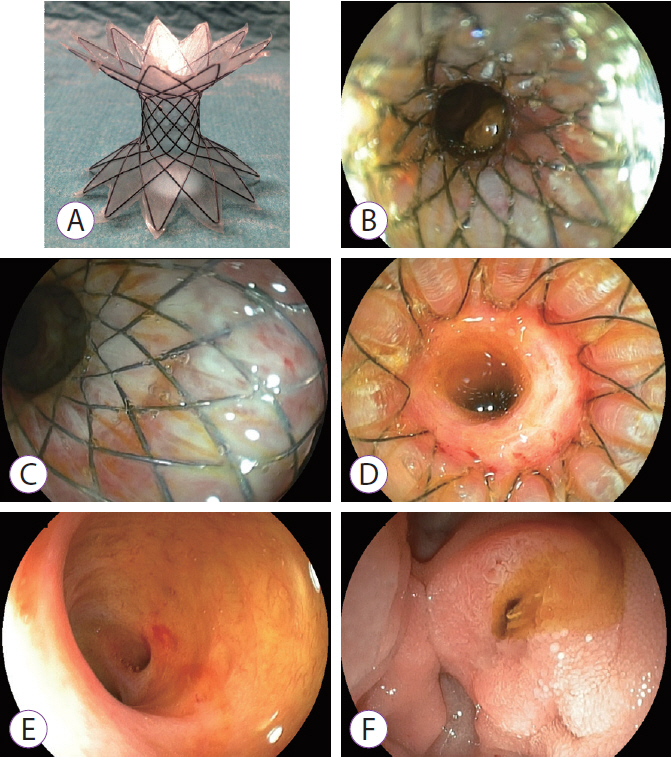
Here, I present a novel approach of using upfront transpapillary LAMS for symptomatic stone disease and through-the-LAMS direct cholangioscopy (DC) access. Following non-ST-segment elevation myocardial infarction and drug-eluting stent implantation in an elderly patient, index endoscopic retrograde cholangiography (ERC) performed six weeks earlier revealed several small bile duct stones, and 7-F plastic stenting was performed. At repeat ERC, a 30├Ś10-mm yoyo-type LAMS (Diabolo stent; Leufen Medical, Berlin, Germany; Fig. 1A) was inserted through the papilla under peri-interventional ceftriaxone and after prophylactic pancreatic duct stenting, with some small stones retained proximal to the stent saddle (Fig. 1B). Using an ultra-slim upper endoscope, through-the-LAMS DC was performed after full stent expansion the next day, showing whitened papillary mucosa due to tissue tension (Fig. 1C), and a tight funnel-shaped adaptation of the proximal stent end to the distal bile duct contour (Fig. 1D). Residual stones were excluded by cholangioscopy, suggesting spontaneous passage after stent expansion (Fig. 1E). Following this, the LAMS was orally extracted without bleeding complications, while the papillary orifice revealed ample spontaneous bile flow (Fig. 1F, Supplementary Video 1). The subsequent course was uncomplicated, and the patient was discharged home.
Metal stenting for the treatment of complex stone disease has been increasingly reported, opening avenues for incisionless procedures with a covered self-expandable metal stent (SEMS) and prolonged stent indwelling duration [2-4]. In contrast to the reported strategies involving a conventional SEMS, a funnel-shaped LAMS may facilitate spontaneous stone passage and may serve as a temporary incisionless access port to the biliary tract for instrumentation and/or performance of DC. Moreover, transpapillary LAMS use has recently been described for management of post-incision bleeding [5]. Upfront LAMS use for spontaneous and/or device-assisted duct clearance followed by cholangioscopic confirmation is a novel and appealing approach for management of common bile duct stone disease in patients on DAPT. However, further technique refinement and systematic study are needed.