INTRODUCTION
Achalasia is a neurodegenerative motility disorder that is caused by impaired relaxation of the lower esophageal sphincter (LES), increased LES tone, and absent peristalsis of the esophagus [1]. Peroral endoscopic myotomy (POEM) is known to be a safe and effective approach for patients with esophageal achalasia compared to surgical treatment. Inoue et al. introduced POEM in 2009 as a non-surgical approach to treat a patient with esophageal achalasia in response to rapidly increasing less invasive treatment requirements [2,3]. Currently, POEM is considered as the first treatment for achalasia, and the indications for POEM have been expanding to sigmoid-shaped achalasia [4].
The POEM procedure for sigmoid-shaped achalasia is more difficult than for other non-sigmoid-type achalasia. The sigmoid-shaped esophagus is considered to a highly advanced achalasia, in which the lumen of the esophagus is significantly rotated with dilatation [3]. As such, advanced achalasia requires other treatment approaches. Here, we report a new technique that is divided between two tunneling sites in the esophagus with flexion, termed тtwo-stage POEMт for sigmoid-type achalasia.
CASE REPORT
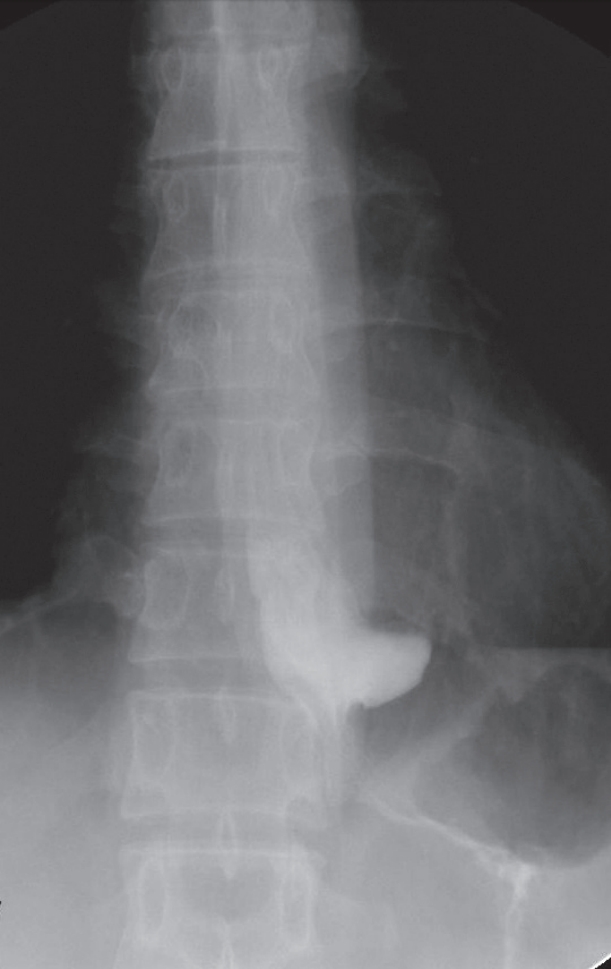
A 40-year-old man visited our hospital with dysphagia that had gradually worsened over the 10 years prior to the visit. He had no known underlying disease or significant family history. On the first esophagogastroduodenoscopy at admission, his esophagus showed retention of fluid and food materials with severe dilatation. He had an Eckardt symptom score of 8. During a barium esophagography, a significant amount of contrast agent remained in the esophagus after 5 minutes and showed a typical bird beak appearance (Fig. 1A). In high-resolution manometry, the integrated relaxation pressure was 11 mmHg, and the patient was subsequently diagnosed with type I achalasia with a sigmoid-shaped esophagus (Fig. 1B).
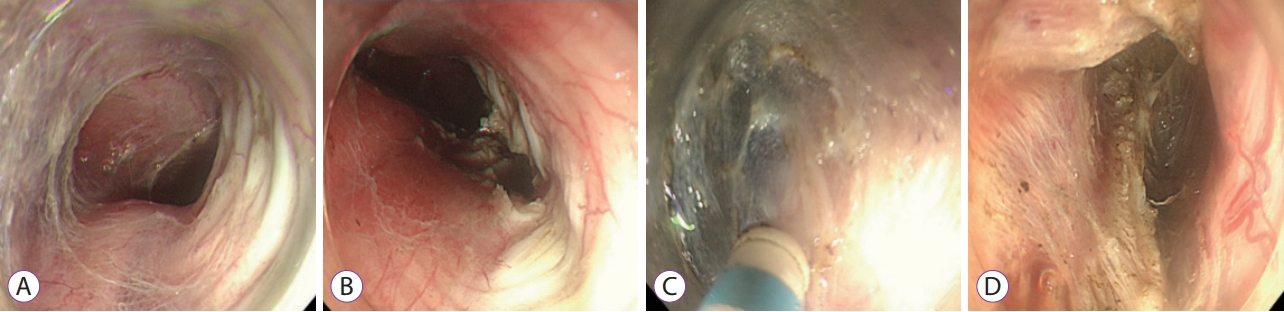
After the general anesthesia, intravenous antibiotics were administered before POEM. A 9.8-mm diameter high-definition esophagogastroscope (GIF-H260; Olympus, Tokyo, Japan) was used for the procedure. The mucosal incision was performed 33 cm from the upper incisors. As in the case of general POEM, myotomy of the inner circular muscle was made by using an IT knife and an F knife. First, a submucosal tunnel was made after a submucosal saline injection using an endoscopic knife in the upper part of the greater flexion area (Fig. 2A), and then myotomy was performed in this area (Fig. 2B). Subsequently, a second submucosal tunnel was made, and myotomy was performed again in the lower part of the flexion (Fig. 2C, D). Finally, endoclipping was used for closure. We termed this method тtwo-stage POEMт, which was successfully performed without any complications (Supplmentary video 1). The procedure time was 85 min and the myotomy length was 10 cm (esophagus, 8 cm; stomach, 2 cm).
Three days later, postoperative esophagography showed the rapid passage of barium from the esophagus into the stomach (Fig. 3). The following day, the patient was discharged from the hospital, and his Eckardt symptom score was reduced to 1 at 6 months after the treatment.
DISCUSSION
POEM has been demonstrated in several studies as an effective treatment for esophageal achalasia, but it remains controversial due to insufficient data from randomized controlled trials and a relatively short follow-up period [4]. Recently, since the therapeutic range of POEM has expanded, a new technological approach may present challenges in endoscopic treatments. Especially in cases of complicated esophageal achalasia, such as progressive sigmoid-shaped esophagus, a new technique is required because it is difficult to perform POEM in such cases. First, a submucosal tunnel is difficult to create without mucosal damage at the site of flexion. Secondly, the expanded and curved esophageal lumen may cause out of direction, and subsequent endoscopic dissection and detachment of the tissue surface is difficult.
Furthermore, patients with previous interventions show inflammation and fibrosis of the submucosal layer, which can interrupt submucosal tunneling. In a cohort study, submucosal fibrosis has been shown to be the most common cause of technical failure of POEM, and this often occurs when there is a history of interventions [5]. They also found that any type of procedure could cause fibrosis, including general benign pneumatic dilation and botulinum toxin injection. A severe angulation also causes difficulties in establishing the mucosal tunneling direction. Lv et al. reported that a deep mucosal tunneling can help maintain the correct distal orientation of the mucosal tunnel by ensuring a direction perpendicular to the circular muscle fibers [3]. Peroral endoscopic full-thickness myotomy has been attempted and reported to be effective for treatment. However, in this study, the overall reflux complication rate of POEM for sigmoid-shaped achalasia was 25.8% [3]. Morphological changes in the esophagus can make endoscopic tunneling more difficult and time consuming [6,7]. Liu et al. investigated the тopen POEMт, which was performed directly without a submucosal tunnel to treat sigmoid-type achalasia [7] and was successfully performed without procedural side effects, resulting in a post-open POEM Eckardt score of 2. These cases have even reported the technical efficacy and feasibility of POEM in patients with advanced achalasia; however, these cases are especially challenging and only experienced operators should perform these procedures.
As shown above, various new therapeutic approaches have been tried during POEM procedure for sigmoid-shaped achalasia. Here, we devised a two-stage myotomy technique. During the procedure, the mucosa is supported by the outside of the tunnel. Unexpected mucosectomy is one of the biggest problems when making the tunnel because patients with achalasia experience chronic inflammation of the mucosa. In particular, patients with sigmoid-type achalasia are more prone to flexion, resulting in more complications. If myotomy is performed first on the upper part of the flexion, the flexion site becomes wider, and subsequently, myotomy of the stomach can be performed more easily. In this patient, the procedure was completed successfully using this method. The procedure time was not long compared to other POEM procedures. However, a comparative study including more patients is needed to determine if this method is more useful and safe for sigmoid-type achalasia.
In conclusion, the symptoms of patients with achalasia who have structural deformities that can result in high chance of treatment failure can be improved using with тtwo-stage POEMт method.