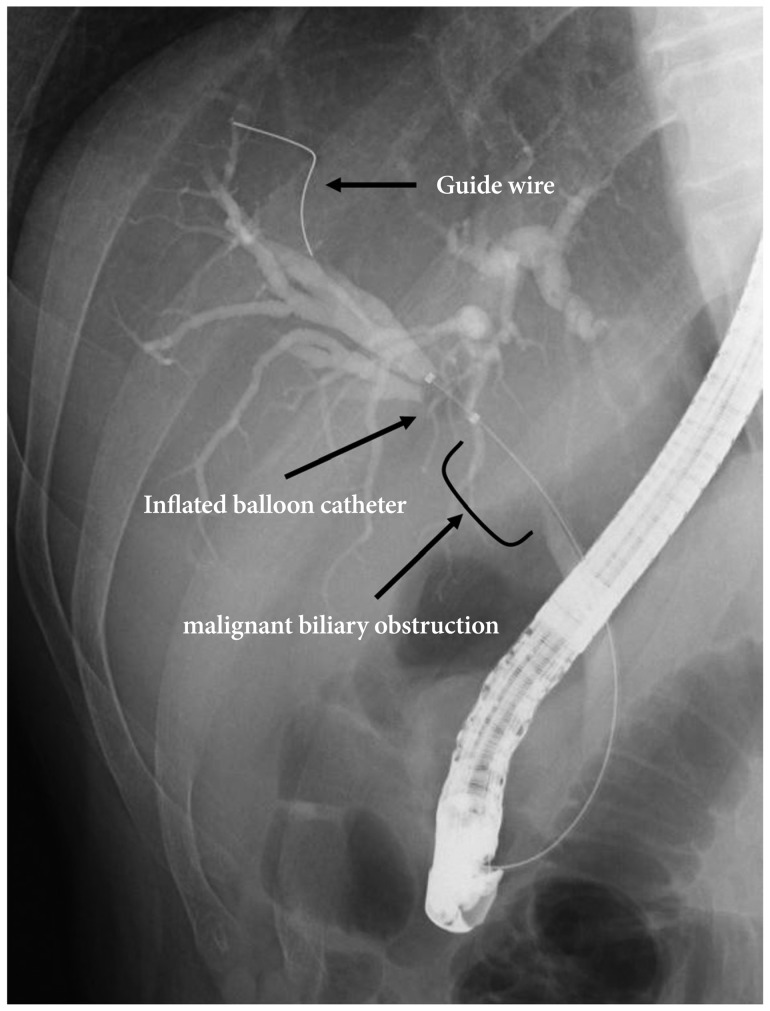
Endoscopic biliary stenting is widely used to palliate malignant obstruction or to treat benign biliary diseases. The technique is less invasive and guarantees high clinical success rates with low morbidity.1,2 In particular, a precise measurement of the length of stenotic area from the papilla makes it possible to place the stent successfully under fluoroscopic monitoring. Although previously taken abdominal computed tomography or magnetic resonance cholangiopancreatography might be helpful, simultaneous measurement using dedicated instruments during endoscopic retrograde cholangiopancreatography can be clinically most helpful.3 For this purpose, we employed a balloon catheter marked with a scale that allowed us to make direct endoscopic measurement of the length from the stenotic area to the papilla. The balloon catheter (Escort II double lumen extraction balloon; Cook Endoscopy, Winston-Salem, NC, USA), marked in advance with a scale, was one that we generally used as a retrieval catheter for biliary stone extraction. The followings are the step-by-step methods for measuring the length from the stenotic area to the papilla and stent insertion: 1) After the biliary stenosis was identified with cholangiography, a guide wire was inserted in advance through the stenosis; 2) The balloon catheter could pass through the stenosis over the guide wire and advance far enough along to pass the proximal margin of the stenosis; 3) Once the inflated balloon catheter was pulled back until it reached the proximal end of the stenosis (Fig. 1), we could endoscopically measure the length from the stenotic area to the papilla with the scale marked on the balloon cathether (Fig. 2); 4) After removing the balloon catheter, leaving the guide wire, a stent of adequate size was positioned through the stenosis.