INTRODUCTION
In cirrhotic patients, the most common complication is portal hypertension, defined as a pathologic increase in portal venous pressure. Portal hypertension occurs with increased resistance to portal flow in association with increased portal venous blood flow caused by splanchnic vasodilatation [1]. In this condition, collaterals are usually generated to reduce the increased portal pressure and blood flow. Gastroesophageal varices (GOVs) are the most significant collaterals, and they could grow and finally rupture with the aggravation of portal hypertension [2].
Acute hemorrhage from GOVs is one of the most lethal complications of portal hypertension and a leading cause of mortality in cirrhotic patients [3]. Thus, the initial management of acute variceal bleeding is crucial, which is broadly divided into the following categories: (1) general management including resuscitation, vasoactive agents, and prophylactic antibiotics and (2) therapeutic endoscopy. General management is well defined in the recent guidelines [4,5]. Patients with acute variceal bleeding should be treated in the intensive care unit to maintain the circulatory and respiratory status. For restoring hemodynamic stability, packed red blood cell transfusion should be initiated, with a target hemoglobin level of 7ŌĆō9 g/dL. For reducing portal pressure, intravenous infusion of vasoactive drugs, including somatostatin, terlipressin and octreotide, should be administered in combination with therapeutic endoscopy, with the infusion continued for 3ŌĆō5 days. Bacterial infection frequently occurs in cirrhotic patients with upper gastrointestinal (GI) bleeding and is related to high mortality rates. Recent guidelines recommend antibiotic prophylaxis in all cirrhotic patients with acute variceal bleeding. The best antibiotic choice is intravenous 1 g ceftriaxone every 24 h for a maximum of 7 days.
In the last three decades, bleeding-related mortality has decreased from about 50% to 15%ŌĆō20% owing to the standardization of supportive care and advances in endoscopic treatment and radiologic intervention [5]. This review focuses on the currently available endoscopic therapy and radiologic intervention for acute GOV bleeding based on recent studies.
TIMING OF ENDOSCOPY FOR VARICEAL BLEEDING
It is generally accepted that upper GI endoscopy should be conducted to identify variceal hemorrhage in cirrhotic patients with hematemesis [6]. However, the optimal timing of endoscopy remains undetermined. One retrospective study showed that bleeding-related mortality was not associated with the timing of endoscopy in hemodynamically stable condition [7]. In contrast, two studies reported that the mortality rate was lower in patients with early endoscopic treatment than in those with delayed endoscopic treatment [8,9]. Although the optimal timing of endoscopy could not be confirmed, recent guidelines recommend that endoscopy should be conducted within 12 h in cirrhotic patients with acute upper GI bleeding [5,6].
MANAGEMENT OF ESOPHAGEAL VARICEAL BLEEDING
Esophageal varices
About 30%ŌĆō40% of cirrhotic patients with compensated liver function have esophageal varices (EVs), while approximately 85% of patients with decompensated cirrhosis have EVs. The 1-year rate of a first variceal bleeding is about 10%ŌĆō15%. About 60% of patients experience recurrent variceal bleeding within 1 year in the absence of proper treatment [5].
In the thoracic esophagus, venous drainage to systemic veins mainly occurs through the azygos and hemiazygos venous system. In contrast, the abdominal esophagus predominantly drains into the portal venous system through the left gastric vein and partly to the inferior vena cava through the superior and inferior phrenic veins. With reversal flow in portal hypertension, the left gastric vein generally acts as the afferent vessel providing blood to EVs in patients with cirrhosis.
Endoscopic management
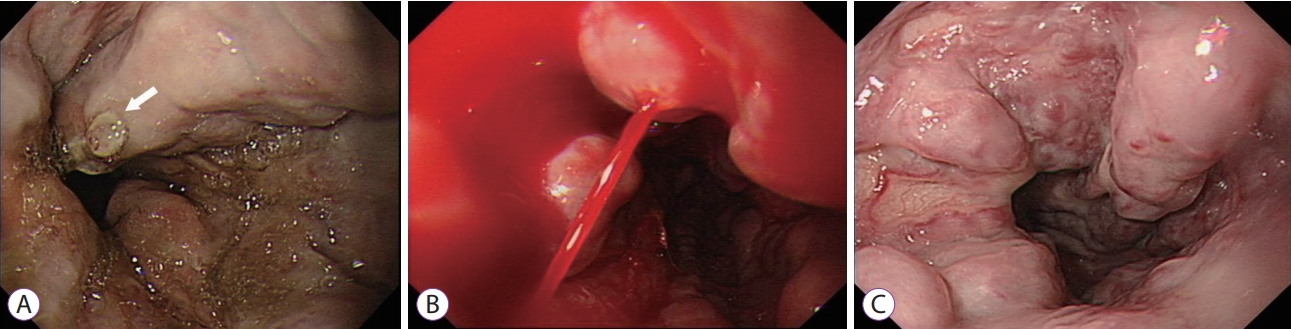
The endoscopic diagnosis of esophageal variceal hemorrhage depends on the presence of varices with a white nipple sign (Fig. 1A) or active bleeding (Fig. 1B). The blood in the stomach and large varices with red wale marks (Fig. 1C) in the absence of other potential sources of bleeding are also considered evidence of esophageal variceal hemorrhage [10]. Endoscopy should be conducted as soon as possible, preferably within 12 hours, in cirrhotic patients with hematemesis. If variceal bleeding is suspected, endoscopic therapy should be performed. The aim of endoscopic therapy for EV is to decrease variceal wall tension through variceal obliteration. The endoscopic modalities for treating esophageal variceal hemorrhage are endoscopic injection sclerotherapy (EIS) and endoscopic variceal ligation (EVL).
EIS involves the injection of a sclerosing agent including sodium tetradecyl sulfate, ethanolamine oleate, or absolute alcohol into the variceal lumen or adjacent to the varices. Injected sclerosing agents cause injury to endothelial cells, destruct the red blood cells, and result in thrombosis of varices [11]. For complete obliteration of the varices, repeated sessions should be performed. Before EVL, EIS was the first-line treatment for esophageal variceal bleeding, as it was proven to be superior to balloon tamponade or vasoconstrictor administration in terms of bleeding control. However, EIS is no longer considered as standard treatment because it has a higher rate of treatment failure and more complications than EVL [12,13].
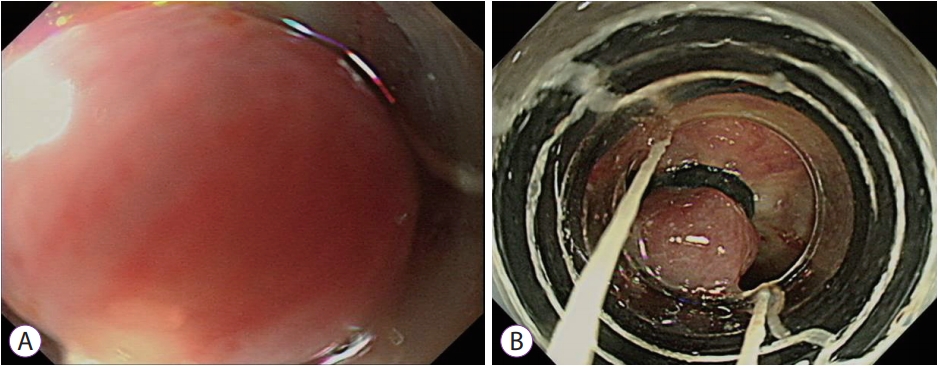
Currently, EVL is considered the gold standard therapy for esophageal variceal bleeding [6]. Contrary to EIS that involves chemical obliteration, EVL eradicates varices through mechanical strangulation with rubber bands. In EVL, variceal columns are sucked into a transparent cap mounted on the tip of the endoscope and ligated with rubber bands. Multiband devices are more commonly employed than the original single-band ligators because multiband devices are much simpler and quicker to use and do not need an overtube [14]. Once the varix is identified, the tip of the endoscope is pointed toward the varix, which is then continuously sucked into the transparent cap. During the suctioning of the varix into the cap, the rubber band can be fired when a ŌĆ£red-outŌĆØ sign appears (Fig. 2A, B) [15]. Generally, the procedure is conducted by starting the deployment of the bands at the gastroesophageal junction and working upwards in a spiral pattern to prevent overlapping circumferential deployment of bands at the same level [11]. It is better to place at least one band on each distinct variceal column. In the presence of active bleeding, the field of vision might be restricted by the cap mounted on the tip of endoscope. Water infusion and suction can help in visualizing the bleeding focus. If possible, the rubber band should be deployed at the site of variceal bleeding. However, if the bleeding point cannot be confirmed, blind multiband ligations at the gastroesophageal junction may sufficiently reduce hemorrhage to obtain a field of vision and subsequently performing proper ligation [15,16]. Currently, the Baveno VI guidelines recommend that patients presenting with acute variceal bleeding should be treated with a combination therapy of EVL and vasoactive drugs [6].
Management of patients with endoscopic hemostasis failure
As failure to control bleeding leads to death, it indicates the necessity to change the treatment option. Hemostasis failure is defined by one of the following criteria occurs within 5 days of an acute bleeding episode: (1) Ōēź100 mL fresh hematemesis for 2 h after the initiation of therapeutic endoscopy, (2) occurrence of hypovolemic shock, and (3) 3 g/dL decrease in hemoglobin within any 24 h period without transfusion [4].
In patients with standard treatment failure, the transjugular intrahepatic portosystemic shunt (TIPS) is considered the best rescue treatment.17 This procedure is performed to establish a low-resistance tract between the hepatic vein and the portal vein through an angiographic technique (Fig. 3A, B). The patency of the tract is maintained by placing an expandable metal stent, thereby permitting blood to flow directly from the portal vein to the systemic circulation. TIPS controls variceal hemorrhage by decompressing the portal pressure. In a prospective study conducted in 58 patients as soon as possible after the diagnosis of refractory variceal hemorrhage, the efficacy of salvage TIPS was higher than that of EIS combined with vasoactive drugs. After salvage TIPS, variceal bleeding was controlled in 52 of 58 patients (90%), and the survival rate was 51.7% and 40.2% at 1 year and 3 years, respectively [17]. The major cause of variceal rebleeding after TIPS is obliteration or stenosis of the stent. Since the introduction of polytetrafluoroethylene-covered stents, markedly improved longterm stent patency compared with bare metal stents has been achieved [18,19].
Balloon tamponade, which uses a nasogastric tube with two inflatable balloons attached (for the esophagus and stomach), showed high hemostasis efficacy in patients with acute esophageal variceal hemorrhage, whereas Ōēź50% of patients experienced rebleeding after deflation [20]. In addition, because it is related to serious adverse events such as aspiration pneumonia, as well as ulceration or perforation of the esophagus, the deployed balloon should not be retained for >24 h. Thus, balloon tamponade should only be considered in massive hemorrhage as a short-term bridging therapy before a more definite treatment such as TIPS [4].
MANAGEMENT OF GASTRIC VARICEAL BLEEDING
Gastric varices
Compared with EVs, gastric varices (GVs) have lower incidence and bleeding rate [21]. However, gastric variceal bleeding is usually more massive, requires more transfusions, and is related to higher rebleeding and mortality rates than esophageal variceal bleeding [3,21,22].
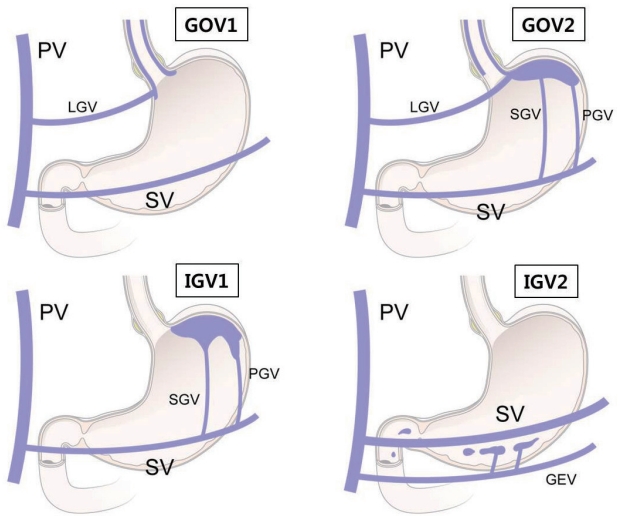
The Sarin classification system is the most widely used and practical method for risk stratification and treatment of GVs (Fig. 4) [21]. GVs are categorized into GOVs and isolated GVs (IGVs) based on the association of GVs with EVs. According to their location in the stomach, GOVs and IGVs are both subclassified into type 1 and type 2. GOVs are a continuation of EVs spreading out either into the lesser curvature (GOV1s) or the fundus along the greater curvature (GOV2s). IGV1s are situated in the fundus of the stomach and IGV2s are isolated ectopic varices that are present at any location in the stomach except the fundus or the intestine. Hemodynamically, EVs and GOV1s arise from the left and right gastric veins, whereas IGV1s and GOV2s are usually supplied by the short and posterior gastric veins [23]. IGV2s are supplied by the gastroepiploic veins [24]. The risk of bleeding is significantly higher in fundal varices than in either GOV1s or IGV2s [21].
Endoscopic treatment for GOV2 and IGV1 bleeding
GOV2s and IGV1s are collectively called fundal varices and supplied by the short and posterior gastric veins [23]. Fundal variceal bleeding commonly occurs in large varices and is accompanied by a gastrorenal or splenorenal shunt [25]. Because fundal varices have a large volume and fast flow of blood, bleeding control is difficult and the rebleeding rate is high.
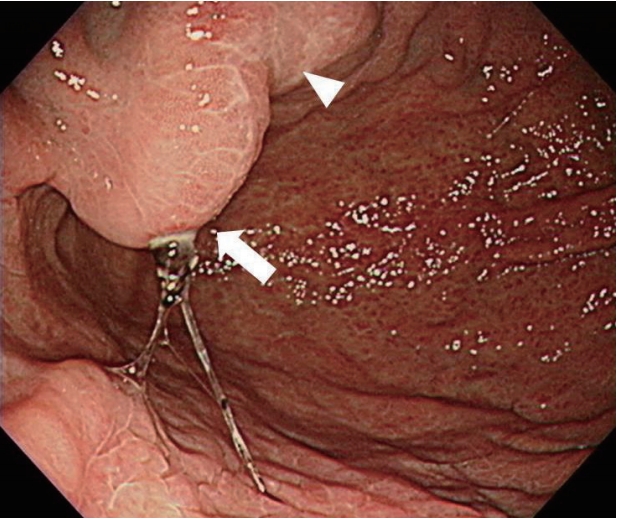
Endoscopic variceal obturation (EVO) is the therapeutic endoscopy method of choice for acute bleeding from GOV2s and IGV1s [4,26,27]. GVs are obturated by injecting a tissue adhesive agent, such as cyanoacrylate, which leads to solidification and thrombosis in the varices [24]. Contrary to sclerosing agents used in EIS, which induce thrombosis and fibrosis of varices through endothelial damage, cyanoacrylate is rapidly transformed into a hard plastic material within varices, resulting in their solidification and thrombosis. The standard protocol uses a mixture of cyanoacrylate and Lipiodol in a 1:1 ratio to delay premature hardening. The mixture of cyanoacrylate and Lipiodol is directly injected into the GVs at 1ŌĆō2 mL each time with a needle catheter. Immediately after injection, distilled water should be passed to deliver the cyanoacrylate from the dead space of the catheter lumen to GVs. Before the procedure, the dead space of catheter lumen should be checked to confirm the volume of distilled water for flushing. The needle should be promptly extracted after cyanoacrylate injection to prevent it from being embedded in the varix. After extracting the needle, distilled water should be passed into the catheter lumen at high speed for 15ŌĆō20 s to prevent closure of the catheter lumen. Until the varix is hard enough to touch with a needle catheter, repeated injection could be performed [28]. When deciding the site of injection, the direction of variceal blood flow and the variceal size should be considered. Huge fundal varices have a large volume and rapid flow of blood from the cardia to the fundus. Theoretically, the dome of the varix has the highest pressure and fastest blood flow. Thus, the most protruding portion or the nipple sign of the varix should be avoided to prevent massive bleeding. Therefore, it is safer to inject at the branch of the cardia area, which has lower pressure (Fig. 5) [29]. After EVO therapy, cyanoacrylate gradually causes an inflammatory response and eliminates vascular endothelial cells, causing variceal obliteration. The complications that could occur after EVO are fever, infection, perforation, gastric ulcer, and peritonitis [28]. Severe complications are mostly associated with distant embolic events such as pulmonary, cerebral, and splenic infarction [30]. In several studies evaluating the efficacy of EVO for acute gastric variceal bleeding, the success rate of hemostasis was 91%ŌĆō97% and the rebleeding rate was 17%ŌĆō49% at 1 year [31-33]. A recent meta-analysis reported that EVO achieved a significantly higher hemostasis success rate (odds ratio [OR], 4.44; 95% confidence interval [CI], 1.14ŌĆō17.3) and a lower rebleeding rate (OR, 0.06; 95% CI, 0.01ŌĆō0.58) than EVL [34].
Endoscopic treatment for GOV1 bleeding
GOV1s are more similar to EVs than GOV2s and IGV1s in terms of size and route of portal blood flow, including having a smaller size than fundal varices as well as afferent venous drainage through the left and right gastric veins. GOV1s are closely connected with EVs because obliteration of EVs with EVL or EIS frequently induces resolution of GVs in 60%ŌĆō65% of patients with GOV1s [21,35]. Therefore, GOV1s are usually treated with EVL, similar to EVs. However, GOV1s are present in the stomach where the overlying mucosal layer is thicker than that in the esophagus. The thick overlying mucosal layer of GVs could result in incomplete ligation of varices with EVL, which could induce massive hemorrhage after detaching the rubber band from the stomach mucosa [36,37]. Furthermore, bleeding from post-EVL ulcers could occur more frequently in the stomach than in the esophagus ¾░üø38]. In fact, EVO seems to be superior to EVL in treating acute bleeding from GOV1s. In several randomized controlled trials and retrospective studies, the success rate of hemostasis was 85%ŌĆō100% with EVO and 80%ŌĆō90% with EVL, and the rebleeding rate was 3%ŌĆō26% with EVO and 14%ŌĆō56% with EVL [35,38-40]. In addition, a recent meta-analysis showed that the efficacy of EVO was superior to that of EVL in preventing rebleeding from GOV1s (OR, 0.39%; 95% CI, 0.16ŌĆō0.94; p=0.035) [34]. In summary, both EVO and EVL are available treatment options; however, EVO is preferred over EVL.
Radiologic intervention for the management of acute and refractory gastric variceal bleeding
From the point of view of interventional radiologists, the main modalities available for the treatment of GVs are TIPS and balloon-occluded retrograde transvenous obliteration (BRTO).
TIPS induces hemostasis of gastric variceal bleeding and decreases the risk of rebleeding by decompressing the portal pressure. In two retrospective studies comparing TIPS and EVO in patients with fundal variceal bleeding, the hemostasis rate was Ōēź90% with both TIPS and EVO; however, TIPS had more adverse effects such as hepatic encephalopathy and stent stenosis, and was more expensive than EVO [41,42]. Therefore, TIPS could be an optimal choice in patients with gastric variceal hemorrhage refractory to medical and endoscopic treatment. In several studies assessing the efficacy of salvage TIPS for refractory gastric variceal hemorrhage, the hemostasis rate was 90%ŌĆō100% and the rebleeding rate was 16%ŌĆō40% [43-46].
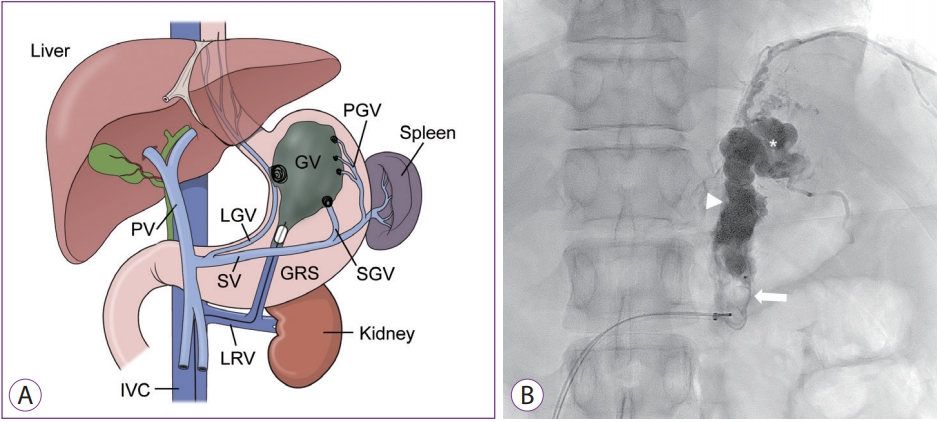
BRTO is a radiologic technique that involves thrombotic obliteration of GVs by instillation of a sclerosing agent into the GV via the gastrorenal or gastrocaval shunt while an inflated balloon occludes the blood flow of the varix (Fig. 6A). Before the procedure, the presence of a spontaneous gastrorenal or gastrocaval shunt should be confirmed with contrast-enhanced computed tomography of the abdomen. Patients with GVs usually have these shunts [23]; however, about 15% of patients with GVs have other portosystemic shunts and BRTO is not available in these patients. In two retrospective studies assessing the efficacy of BRTO for the management of gastric variceal hemorrhage, the success rate of BRTO was 95%ŌĆō97%, although 20%ŌĆō41% of patients showed adverse events causing the worsening or relapse of EVs after BRTO [47,48]. Thus, follow-up endoscopy is needed after BRTO. A recent meta-analysis reported that the technical success rate of BRTO was 96.4% and the clinical success (defined as no recurrence or rebleeding, or complete obliteration of GVs) rate was 97.3% [49]. For the treatment of patients with refractory gastric variceal hemorrhage, the efficacy of BRTO is comparable to that of TIPS [50]. Currently, a modification of BRTO, plug-assisted retrograde transvenous obliteration (PARTO), has been introduced to reduce the complications of BRTO related to the use of a sclerosing agent and a balloon catheter (Fig. 6B). In PARTO, a vascular plug and gelatin sponge are used instead of a balloon occlusion catheter and a sclerosing agent. In a recent multicenter prospective study evaluating the efficacy of PARTO in the treatment of GVs, 98.6% of patients showed complete thrombosis of GVs and gastrorenal shunts within 1 week after PARTO [51]. Procedure-related adverse events, rebleeding of GVs or hepatic encephalopathy were not reported in the follow-up period. For the management of gastric variceal bleeding, PARTO has the potential to replace BRTO.
In summary, TIPS is recommended as a rescue therapy in patients with refractory gastric variceal bleeding. BRTO could be considered as a salvage treatment in patients with refractory hemorrhage of GVs in the case of having a gastrorenal shunt. In the management of fundal variceal bleeding, TIPS and retrograde transvenous obliteration methods such as BRTO or PARTO could be considered as initial hemostatic therapy.
NEW ENDOSCOPIC MODALITIES IN THE TREATMENT OF VARICEAL BLEEDING
Hemostatic powder
Recently, hemostatic powders have been introduced as endoscopic tools for the management of GI bleeding. Hemostatic powder forms a mechanical barrier when it comes into contact with water in the GI tract. Although this technique needs a dedicated delivery system, it requires minimal experience in therapeutic endoscopy. A recent randomized controlled trial evaluated the efficacy of a hemostatic powder for the treatment of acute variceal hemorrhage [52]. In this study, 86 patients with acute variceal hemorrhage were randomized to receive medical and endoscopic therapy within 12ŌĆō24 h of hospital visit or medical treatment and hemostatic powder application within 2 h of hospital visit followed by endoscopic therapy (EVL for esophageal variceal bleeding, EVO for gastric variceal bleeding) within 12ŌĆō24 h. Patients who underwent medical therapy and early hemostatic powder application followed by endoscopic therapy showed significantly reduced clinical rebleeding within 24 h and increased survival rate compared with those who underwent standard medical and endoscopic therapy. This study suggests the role for hemostatic powders as an initial therapy for acute variceal bleeding, especially for endoscopists with in minimal expertise.
Self-expandable metallic stents
Balloon tamponade is effective in controlling refractory esophageal variceal hemorrhage in up to 90% of cases, while the rebleeding rate is Ōēź50% after deflation [20]. In addition, as balloon tamponade is related to serious complications such as ulceration or perforation of the esophagus, as well as aspiration pneumonia, the balloon should not be retained for Ōēź24 h. Self-expandable metallic stents (SEMSs) may provide a useful alternative to esophageal balloon tamponade in patients with refractory acute variceal hemorrhage. In a small-sized randomized controlled trial comparing SEMS with balloon tamponade in patients with refractory esophageal variceal hemorrhage, SEMS showed a higher hemostasis rate (85% vs. 47%, p=0.037) and fewer serious adverse events (15% vs. 47%, p=0.077) than balloon tamponade, although the six-week survival rate was not significantly different between the two treatments [53]. SEMS can be placed and removed endoscopically without fluoroscopy, and can be left in place for up to 2 weeks. This technique could be considered as a bridge therapy to TIPS.
Endoscopic ultrasonography-guided cyanoacrylate and coil embolization
Endoscopic ultrasonography (EUS)-guided vascular embolization has been introduced as a new option for controlling bleeding. In the endoscopic treatment of GVs, EUS has several strengths. Because it provides real-time, high-quality images of the GI wall and vascular structure, EUS is superior to direct endoscopy in detecting GVs [54]. Especially during active bleeding, EUS visualization is not restricted. Thus, the detection rate of GVs is higher and a fast therapeutic procedure is possible. After embolization, EUS can confirm the obliteration of vascular flow in the varix through Doppler assessment.
These strengths might allow EUS-guided therapy combined with cyanoacrylate and coil in patients with gastric variceal bleeding. This procedure consists of the following three steps: (1) EUS-guided puncture of GVs with a fine-needle aspiration (FNA) needle, (2) coil delivery into the varix through the FNA needle, (3) injection of cyanoacrylate via the FNA needle [55]. In this procedure, coil might improve hemostasis with a lower dose of cyanoacrylate and decrease the risk of systemic embolization by acting as a layer for retaining cyanoacrylate. A recent study assessed the efficacy of EUS-guided therapy combined with cyanoacrylate and coil in 152 patients with GVs [56]. The technical success rate was 99%, with a mean coil number of 1.4 and a mean cyanoacrylate volume of 2 mL. In follow-up EUS, 93% of patients showed complete obliteration of GVs (on Doppler study). The rate of systemic embolization was lower in this study (0.7%) than in a previous study with EUS-guided cyanoacrylate injection alone (10.5%). Although this procedure shows promising results, further studies are needed before it can be considered a treatment option for gastric variceal bleeding.
CONCLUSIONS
The treatment of acute variceal bleeding requires a multidisciplinary approach involving medical treatment, endoscopic treatment, and radiologic intervention. For hemostasis against initial and recurrent hemorrhage, therapeutic endoscopy is an important modality. The two main methods of endoscopic hemostasis are EVL and EVO, and the choice between these methods is decided according to the type of varices. In case of endoscopic hemostasis failure, radiologic interventions such as TIPS and BRTO are considered good options for salvage therapy. New endoscopic modalities, including hemostatic powders, SEMS, and EUS-guided therapy might find their position in the treatment of acute variceal bleeding through the future studies.