INTRODUCTION
Acute cholecystitis is one of the most common biliary diseases. Most patients with acute cholecystitis need urgent treatment and sometimes develop severe complications if appropriate drainage is not performed. Therefore, according to the Japanese guidelines [1], early gallbladder drainage is essential in patients with severe (grade II or III) cholecystitis in the presence of multiple organ dysfunction and/or severe local inflammation. The gold standard therapeutic strategy is cholecystectomy; however, surgery may result in increased mortality, especially in elderly patients and/or in those with multiple severe comorbidities [2-7].
The common drainage techniques include percutaneous transhepatic gallbladder drainage (PTGBD) and percutaneous transhepatic gallbladder aspiration (PTGBA), which are well known to be effective methods for primary drainage [8-12]. However, these procedures cannot be adopted in patients with massive ascites, anatomically inaccessible gallbladder [13-15], risk of self-removal of the drainage tube, or bleeding tendency [16-18].
Endoscopic transpapillary gallbladder drainage (ETGBD) is considered to be the second-line drainage procedure for acute cholecystitis. This method has also been reported to have a high success rate and a low complication rate, suggestive of a sufficient degree of efficacy in patients who are not candidates for PTGBD [9-23]; however, some attention should be paid to acute pancreatitis as a representative complication [24]. In addition, this method has a technical limitation and difficulty in that the cystic duct (CD) and the orifice of the CD cannot be enhanced during a cholangiography owing to tortuosity, calculus, or malignant obstruction of the CD [25,26]. In a previous report, we proposed a new method of ETGBD combined with intraductal ultrasonography (IDUS) [27]. With the additional IDUS, the orifice of the CD in the common bile duct (CBD) can be easily detected and CD cannulation may also be easily performed. In the present study, we aimed to evaluate the efficacy and feasibility of ETGBD with IDUS compared with those of ETGBD alone, and to discuss whether this technique can be a standard method for gallbladder drainage in patients with acute cholecystitis.
MATERIALS AND METHODS
Study design
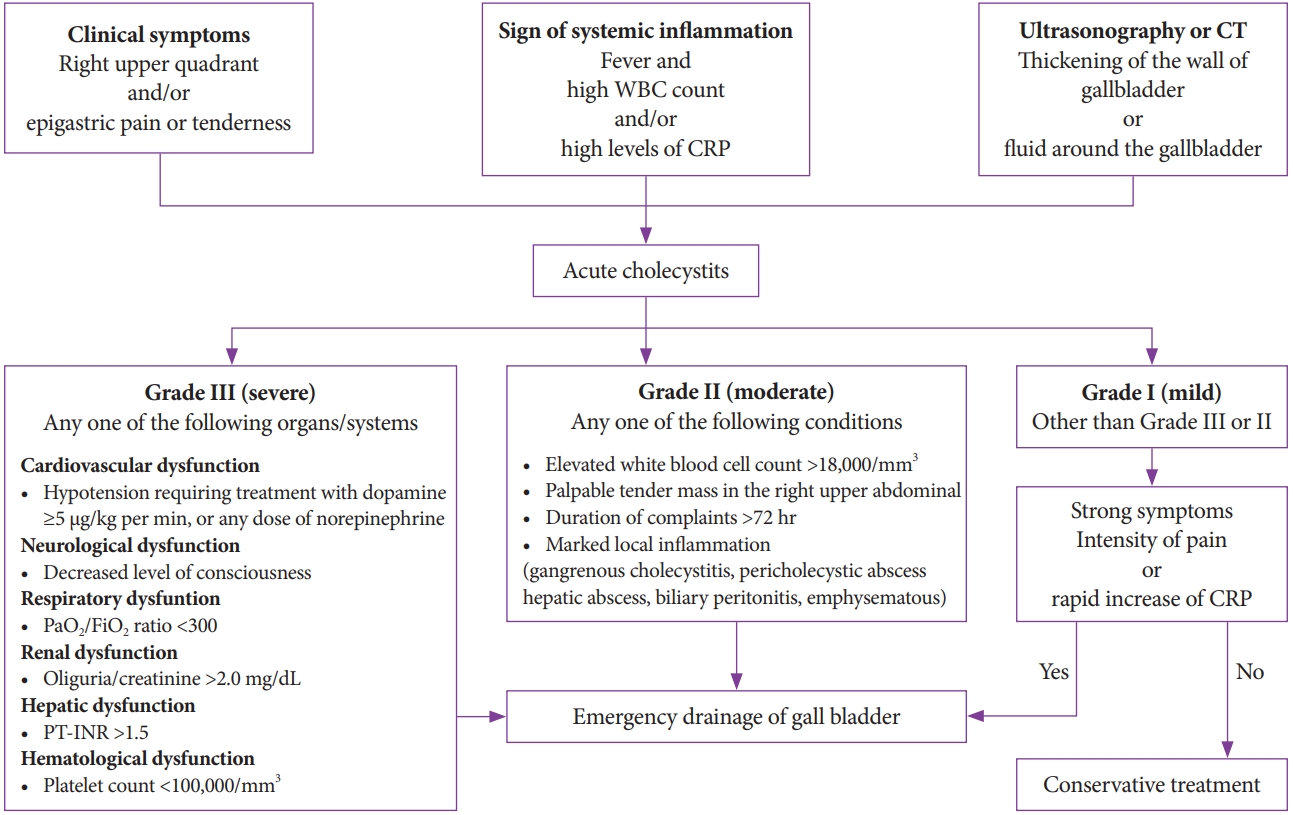
A total of 100 patients with acute cholecystitis requiring ETGBD treatment from January 2015 to December 2017 were retrospectively enrolled in the present study. The first 50 consecutive patients out of the 100 patients were treated using ETGBD without IDUS and the next 50 consecutive patients were treated using ETGBD with IDUS. Acute cholecystitis was diagnosed according to the diagnostic criteria and classified into three grades [1] according to severity and symptoms (Fig. 1).
Patients with grade III (severe) and grade II (moderate) acute cholecystitis required urgent drainage of the gallbladder. Grade I (mild) acute cholecystitis was defined as milder than grade III or II, and accordingly did not require drainage. However, we sometimes performed drainage in patients with grade I acute cholecystitis when their symptoms included intense abdominal pain and/or when they had a significantly severe inflammatory condition in which the C-reactive protein (CRP) level or white blood cell (WBC) count was 1.5 times higher on the second hospital day. ETGBD was first performed as an alternative to cholecystectomy or PTGBD if patients had massive ascites, anatomically inaccessible gallbladder, risk of self-removal of the drainage tube, and bleeding tendency, or if they had been administered oral antithrombotic agents.
Propensity score matching
We compared the usefulness of ETGBD with IDUS with that of ETGBD without IDUS in patients with acute cholecystitis by using propensity score matching to confirm the validity of this retrospective analysis. Propensity scores were calculated using logistic regression analysis. Age, sex, severity of acute cholecystitis, WBC count, CRP level, and presence of gallbladder stones were used as matching factors. After matching, univariate and multivariate logistic regression analyses were conducted. On the basis of the score obtained from each group, patients treated with ETGBD with or without IDUS were matched using calipers of width equal to 0.2 of the standard deviation of the logit of the propensity score.
Techniques of ETGBD and ETGBD combined with IDUS
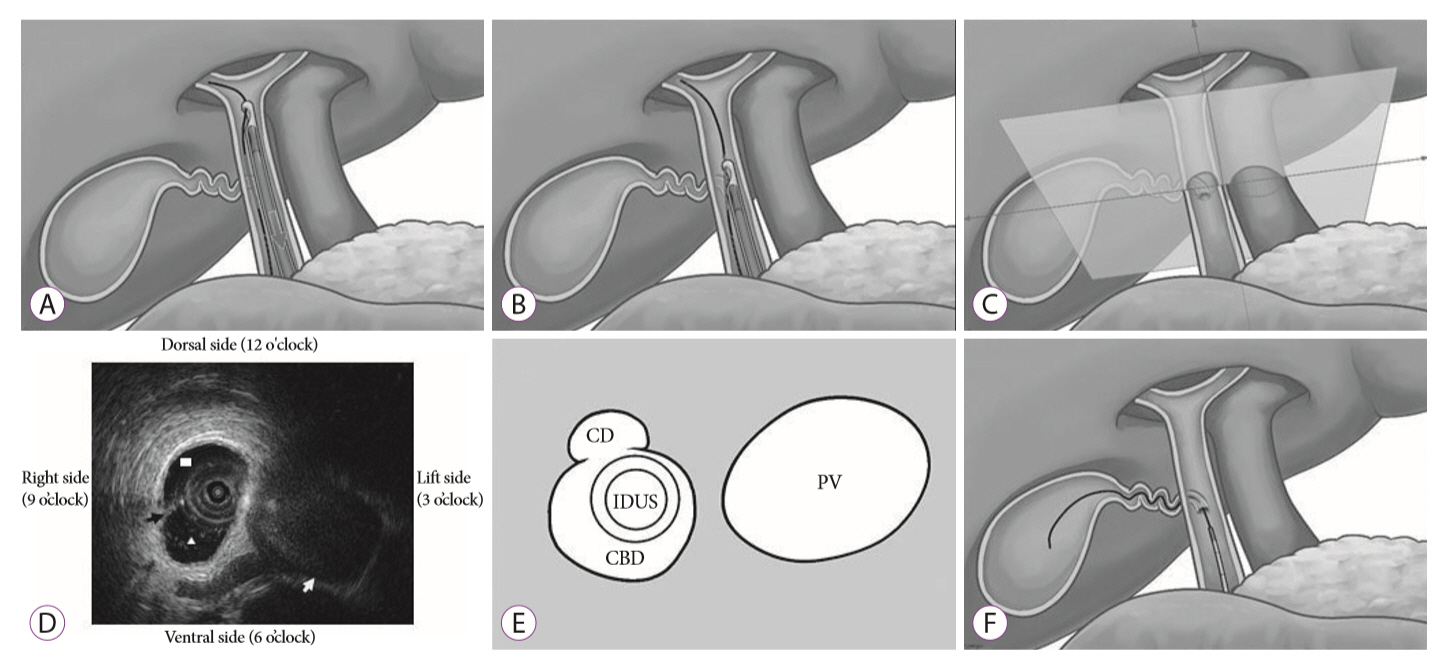
ETGBD was performed using an endoscopic retrograde cholangiopancreatography catheter (MTW; ABIS, Tokyo, Japan) and a 0.025-inch guidewire (VisiGlide 2; Olympus Medical Systems, Tokyo, Japan). After CBD cannulation, endoscopic sphincterotomy or endoscopic papillary balloon dilation was performed. These treatments were considered in patients with a small ampulla of Vater in order to prevent postoperative cholangitis and/or pancreatitis. In the ETGBD without IDUS group, when the CD was imaged with contrast, attempts based on vague clues were made to insert the guidewire into the gallbladder, and a 10-cm, 5- or 7-Fr pigtail stent was placed into the gallbladder. In the ETGBD with IDUS group, the orifice of the CD could be detected using IDUS with the portal vein as a landmark. First, the IDUS probe was inserted into the upper bile duct along a wire under X-ray guidance, and the portal vein was visualized on the IDUS image. While the IDUS probe was slowly pulled out from the upper bile duct to the papilla (Fig. 2A), the CD was detected around the CBD and the partition wall between the CD orifice and the CBD could be identified (Fig. 2B, C). Given that the IDUS image of the portal vein was adjusted to be at the 3 oŌĆÖclock position, the left side of the patient was revealed as the 3 oŌĆÖclock position and the dorsal side was the 12 oŌĆÖclock position (Fig. 2D). The position in which the partition wall became invisible on the IDUS image was the location of the CD branching point (orifice) from the CBD (Fig. 2E). The IDUS position was confirmed with radiography, and this could serve as a guide in performing CD cannulation (Fig. 2F). The procedure for inserting the drainage tube into the gallbladder was as mentioned above.
When ETGBD was a technical failure, PTGBD, PTGBA, endoscopic ultrasound-guided gallbladder drainage (EUSGBD), or elective cholecystectomy was performed.
Outcomes and definitions
First, we compared the technical success of gallbladder drainage, procedure length, and incidence of complications between ETGBD with IDUS and ETGBD without IDUS. Second, we analyzed the clinical efficacy, length of hospitalization, and recurrence rate in patients with acute cholecystitis treated with ETGBD as the first choice. The technical success rate was defined as the rate of successful placement of the catheter into the gallbladder. The procedure length was defined as the time from the first touch of the duodenal papilla to the withdrawal of the endoscope. Clinical efficacy was evaluated on the basis of the number of days requiring WBC normalization, 50% reduction of the CRP level from its peak value, and the start of oral intake. Recurrence was judged to have occurred when acute cholecystitis recurred according to the above-described diagnostic criteria because of stent dysfunction. Early stent dysfunction was defined as stent dysfunction occurring within 14 days after the procedure, and late stent dysfunction was defined as that occurring after 15 days. The clinical success of ETGBD was defined as sufficient improvement of cholecystitis allowing the patient to leave the hospital without stent dysfunction or other complication.
This retrospective study was approved by the Institutional Review Board of New Tokyo Hospital (approval no. 99), registered in the University Hospital Medical Network Clinical Trials Registry (UMIN 000035646), and conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from each patient before enrollment.
Statistical analysis
Categorical variables were analyzed using FisherŌĆÖs exact test or the Žć2 test. Continuous variables were expressed as mean standard deviation and analyzed using StudentŌĆÖs t-test or the Mann-Whitney U-test. Logistic regression analyses were performed using covariates (among those described above) that could potentially influence the success rate of ETGBD, and p<0.05 was considered statistically significant. All data analyses were conducted using SPSS version 24.0 (IBM Co., Armonk, NY, USA).
RESULTS
In the present study, we enrolled 100 patients with acute cholecystitis from January 2015 to December 2017. All of them were selected to undergo ETGBD because of use of antithrombotic therapy, dementia with a possible risk of self-removal of the tube, or a critical complication precluding surgery. Among these 100 patients, the first 50 consecutive patients were treated using ETGBD without IDUS and the next 50 consecutive patients were treated using ETGBD with IDUS. The clinical characteristics of the patients in both groups are shown in Table 1. There were no significant differences in patient characteristics between the ETGBD with IDUS and ETGBD without IDUS groups. Matched pairs (42 patients from the ETGBD without IDUS group and 50 patients from the ETGBD with IDUS group) were analyzed after propensity score matching (Table 1). There were no significant differences in categorical data between the two groups.
A comparison of therapeutic outcomes between the ETGBD with IDUS and ETGBD without IDUS groups is shown in Table 2. The success rate of ETBGD with IDUS was significantly higher than that of ETBGD without IDUS (92% [46/50] vs. 76% [32/42], p=0.044). There was no significant difference in the procedure length between the two groups (66.7 [14ŌĆō215] min vs. 74 [10ŌĆō140] min, p=0.310). The complication rate in the group with IDUS was significantly higher than that in the group without IDUS (6.0% [3/50] vs. 0% [0/42], p<0.001). These complications included mild pancreatitis, bleeding after endoscopic sphincterotomy, and small CD perforation caused by the guidewire. All patients with complications recovered with conservative treatment, and only one case of IDUS technique-related complication was observed. The clinical course after gallbladder drainage of patients in both groups is shown in Table 3. There was no significant difference in patient prognosis between the two groups.
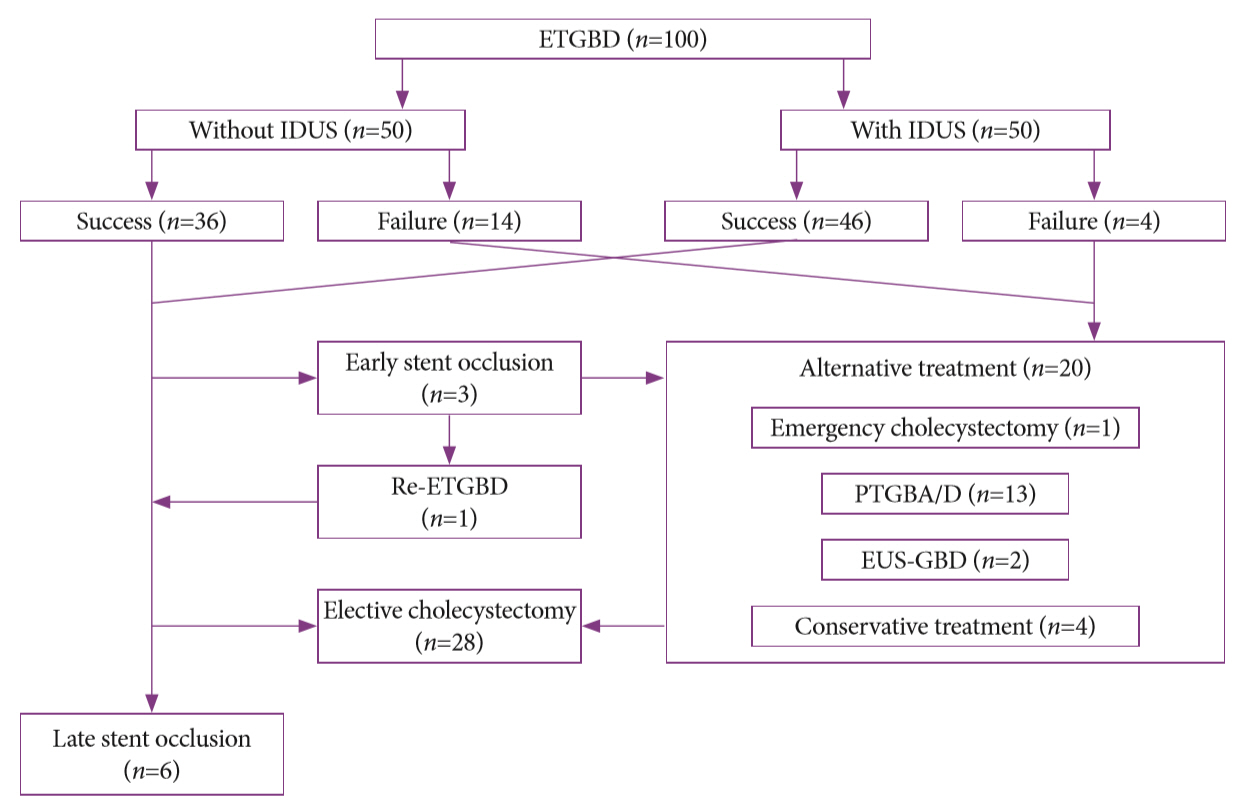
The overall clinical results of ETGBD cases are shown in Fig. 3. The overall technical and clinical success rates of all ETGBD cases were 82% (82/100) and 96% (79/82), respectively. Early stent dysfunction was found in 3.7% of patients (3/82; 1 in the group with IDUS and 2 in the group without IDUS), and ETGBD was successfully re-tried in one patient. Patients who could not be successfully treated with ETGBD (20.0%, 20/100) were alternatively treated using emergency cholecystectomy, PTGBA/PTGBD, EUS-GBD, or conservative treatment including the administration of antibacterial drugs while fasting. Elective cholecystectomy was performed in 28 patients on the next day after the removal of the ETGBD stent. Late stent dysfunction occurred in 7.3% of patients (6/82; 3 in the group with IDUS and 3 in the group without IDUS) after an average observation period of 176 (range, 55ŌĆō337) days.
DISCUSSION
Several studies have reported that ETGBD has a technical success rate of 64%ŌĆō100%, a clinical success rate of 62%ŌĆō100%, and a complication rate of 0%ŌĆō17.2%, representing inter-institutional variances [19-23,28-31]. ETGBD is considered to produce a better therapeutic effect than that of PTGBD especially in patients with massive ascites, anatomically inaccessible gallbladder [13-15], and a possible risk of self-removal of the tube [24]. In addition, this method should be recommended to patients with severe coagulopathy or those receiving antithrombotic therapy when PTGBD is contraindicated owing to a high risk of bleeding complications [16-18].
ETGBD is technically challenging, especially the cannulation step and the passage of the guidewire through the CD. More experience with wire manipulation possibly improves the technical success rate [29]; however, the limitation of ETGBD is its technical difficulty that requires an expert endoscopist to negotiate the CD, especially when the CD cannot be enhanced on a cholangiogram or when the guidewire cannot be inserted through the CD into the gallbladder because of tortuosity, steep angulation, calculus, or malignant obstruction [25,32]. To aim for standardization of ETGBD, some special methods, combined with IDUS [27] or cholangioscopy [33,34], have been previously proposed to make detecting the orifice of the CD in the CBD easier. In general, when the CD or gallbladder is not enhanced on a cholangiogram, CD cannulation becomes more difficult [25,32]. However, our ETGBD combined with IDUS technique possibly improves the negotiation rate of the CD by considering the position of the CD branch level from the CBD even if the CD cannot be enhanced. Consequently, the technical success rate of ETGBD with IDUS was significantly higher than that of ETGBD without IDUS (92.0% vs. 76.0%, p=0.044). This result suggests that the use of IDUS simplifies the negotiation of the CD orifice and does not require the assistance of duct contrast.
Although the procedure length of ETGBD with IDUS was expected to be longer than that of the conventional method, no statistically significant difference in procedure length was observed between the two groups. The complication rate of ETGBD with IDUS was significantly higher than that of the conventional method (6.0% vs. 0%, p<0.001). However, the complications were not serious and resolved quickly with conservative management. Only one case of pancreatitis was observed as an IDUS technique-related complication. In addition, the overall clinical success rate was high (96%). Therefore, it seems that ETGBD with IDUS is a useful and highly effective procedure providing good therapeutic outcomes in patients with acute cholecystitis.
The present study has some limitations. First, the number of enrolled patients was relatively small, although it was not smaller than that of previous studies. Second, the results were possibly affected by the learning curve of the enrolled endoscopists. All ETGBD procedures were performed by two expert endoscopists with experience of >50 ETGBD cases. The procedure length was relatively long because not only the ETGBD procedure itself but also the treatment of the bile duct and pancreatic duct were included in the analysis in this study. The ETBGD procedures without and with IDUS were divided into the first 25 and last 25 cases, respectively, and the technical success rate and procedure length were evaluated in both groups. However, there were no statistically significant differences in these two parameters between the first and last 25 cases. Thus, both parameters were not considered to be affected by the learning curve of the endoscopists.
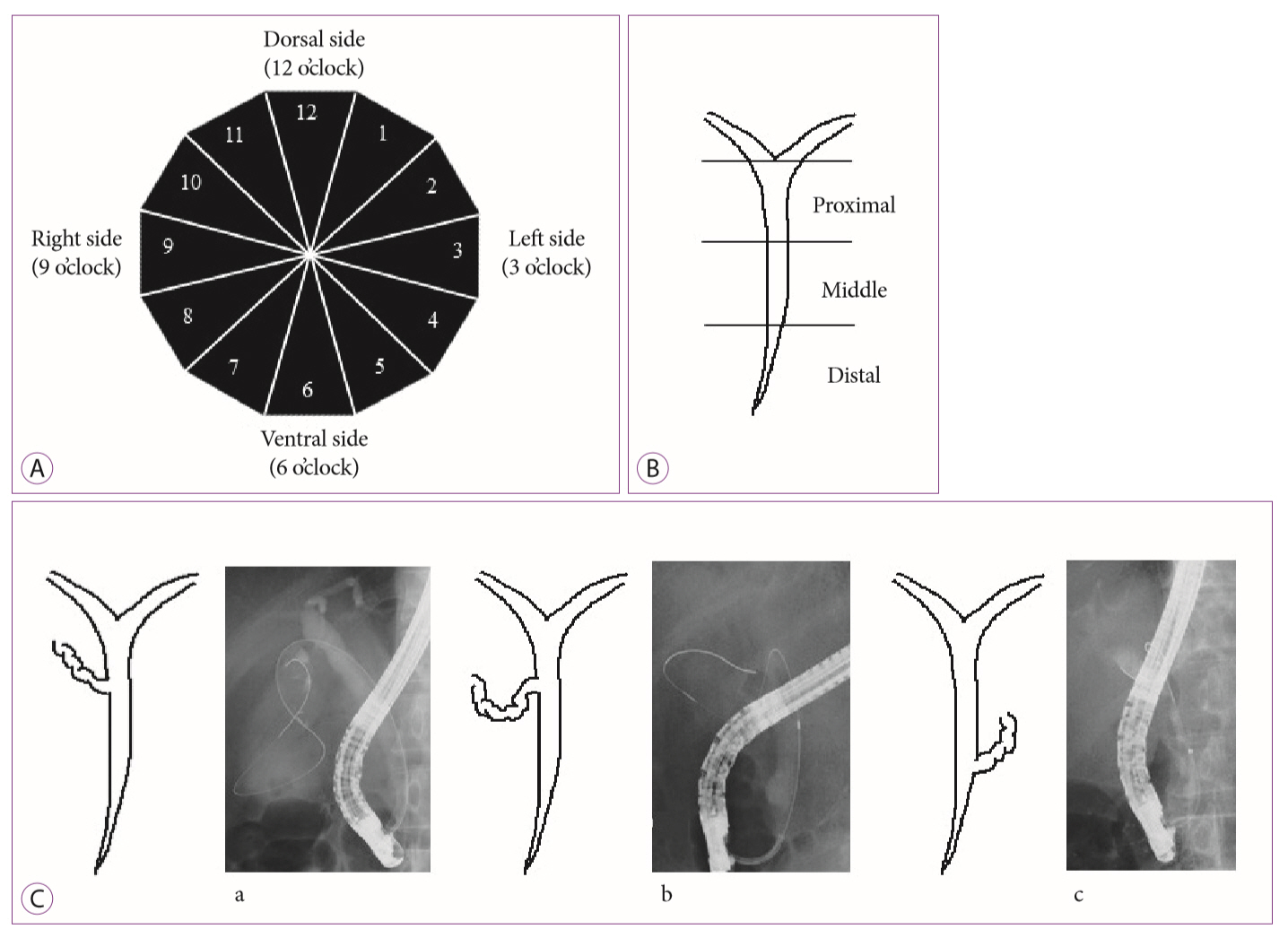
Third, this method requires some special endoscopic techniques owing to anatomical variations of the CD orifice. Such variations possibly make CD cannulation difficult. Therefore, to overcome this technical difficulty, we investigated the position of the CD orifice and the direction of the CD in this study. The oŌĆÖclock position of the direction of the CD orifice was determined in the IDUS image shown in Fig. 4A. The position of the bifurcation of the CD from the extrahepatic bile duct was divided into the following three types: distal, middle, and proximal (Fig. 4B). The CD orifice was also divided into three subgroups based on the location and angle of the orifice (Fig. 4C): right upper (RU) branch (Fig. 4C-a), right downward branch (Fig. 4C-b), and left upper (LU) branch (Fig. 4C-c) types [35-37].
The most frequent branch types were dorsal (11, 12, and 1 oŌĆÖclock positions; 68.0%, 34/50), middle (86.0%, 43/50), and RU (86.0%, 43/50). The success rates of gallbladder stent placement were 88% in the dorsal side, 90.7% in the middle, 93% in the RU branch, 80% in the LU branch, and 100% in the other side (Table 4). This information is considered to be helpful not only for facilitating the cannulation of the CD orifice but also for educating trainee endoscopists. Although this information might also aid CD cannulation, the number of analyzed cases may be too small to draw definite conclusions about the anatomical variations in the position of the CD orifice and the direction of the CD. Further studies with larger numbers of patients are necessary.
In conclusion, ETGBD combined with IDUS is a feasible technique with a high success rate. IDUS may be a useful supportive method for ETGBD and its addition may aid in ETGBD standardization.