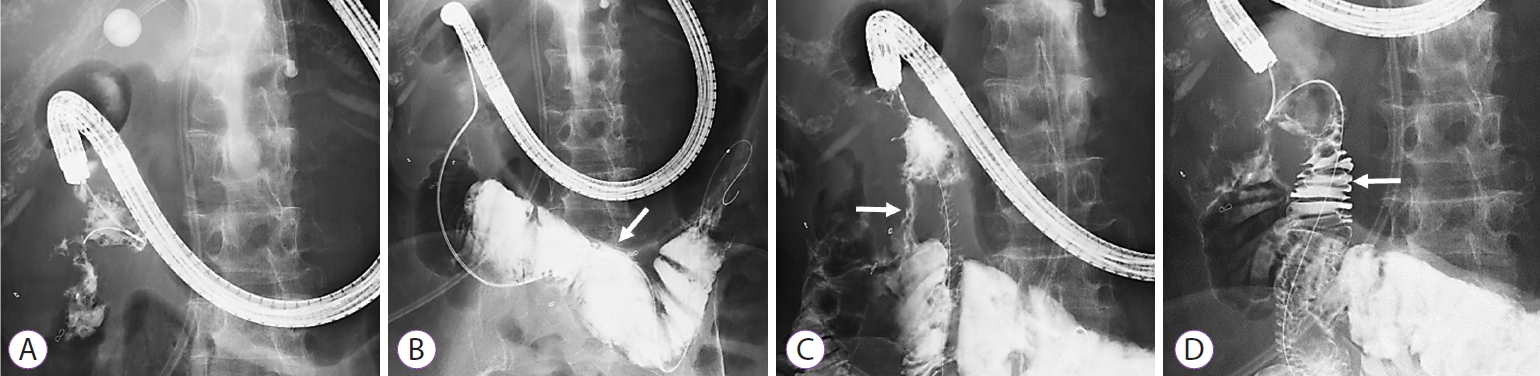
A 57-year-old woman had undergone right hemicolectomy, partial pancreatic head resection, and partial duodenectomy for advanced ascending colon cancer. Owing to a local recurrence, she was referred to our hospital. Percutaneous transhepatic biliary drainage was performed for a malignant biliary obstruction, and the local recurrence was treated with radiotherapy. Systemic chemotherapy was then started, but the patient had a complication of malignant duodenal obstruction 1 year after the recurrence. Only non-contrast-enhanced abdominal computed tomography could be obtained because of the patientŌĆÖs allergy to the contrast medium (Fig. 1). The size of the recurrence site was estimated to be approximately 5 cm. However, detailed information on the occlusion site was difficult to obtain before the endoscopic treatment. A forward-viewing endoscope was inserted in the duodenum, and the guidewire was advanced through the stenosis (Fig. 2A). Subsequent contrast imaging revealed a dilated intestinal tract (Fig. 2B). However, contrast imaging at the stenosis revealed another lumen, and the first lumen was clarified to be the colon, and the guidewire was passed through the duodenocolonic fistula (Fig. 2C). The guidewire was turned to enter another lumen, a true duodenal lumen (Fig. 2D). As the enteral stent was placed at the papilla of Vater, an uncovered enteral stent (NEXENT Duodenal Pyloric Stent 22 mm ├Ś 12 cm; Next Biomedical, Incheon, Korea) was placed at the duodenal obstruction. After the procedure, the patient could take a normal diet (Fig. 3A, B).
Duodenocolonic fistula is a rare complication. It is sometimes caused by benign diseases such as chronic inflammation, a foreign body, and iatrogenic diseases (e.g., those induced by radiotherapy) [1-3]. Duodenocolonic fistula due to malignancy is rare [4]. Furthermore, malignant duodenal obstruction due to colon cancer is unusual. When inserting an enteral stent, the stenosis is passed through using the guidewire under fluoroscopy. The guidewire is confirmed to be inside the intestinal tract based on the contrast image and course of the guidewire. In the case of a duodenocolonic fistula, the obstruction usually occurs at the infraduodenal angle. As the guidewire needs to be advanced to the third portion of duodenum, its course is quite similar to that of the transverse colon. Misplacement of an enteral stent is one of the most critical complications. To avoid this complication, clinicians should be aware that the distal bowel tract below the stenosis is usually collapsed and that no residue-like material is visible. Understanding that the guidewire may go through a lumen different from the assumed duodenum when the fistula is formed is also necessary. The present case of a duodenocolonic fistula was a blind spot in the placement of a duodenal stent. Information on such a case is useful for clinicians who perform enteral stenting.