INTRODUCTION
Tumors of the small bowel are relatively rare in incidence. They account for only approximately 3-6% of all gastrointestinal neoplasms and 1-3% of all gastrointestinal malignancy. Incidence of small intestinal cancer was estimated as 5,300 new cases annually with an estimated 1,100 deaths in the Unites States.1 According to autopsy data, approximately 40 different histological types of tumors arise in the small bowel. The most frequent neoplasms are adenomas and mesenchymal tumors. Less common benign lesions include lipomas, angiomas, and hamartomas. Carcinoid tumor and adenocarcinoma are the most common small intestinal malignancies, with an annual incidence of 3.8 and 3.7 cases, respectively, per million people in the United States, followed by lymphomas (1.1/ million) and sarcomas (1.3/million).2 In Korea, the Annual report of cancer statistics in Korea in 2008 reported the incidence of small intestinal cancer 0.98% of all gastrointestinal malignancy.3 In 2005 United States report,4 the distribution of small bowel cancer histology was 44% carcinoid, 33% adenocarcinoma, 15% lymphoma, and 7% gastrointestinal stromal tumor (GIST). Metastatic small intestinal cancers are from skin melanoma, colorectum, prostate, lung and breast. Multiple factors influence on the relative infrequency of tumorigenesis in the small bowel; rapid small bowel (SB) transit time, a high concentration of the enzyme detoxifying carcinogen,5 abundant lymphoid tissue and high levels of IgA, alkaline pH and the lower bacterial load, and rapid turnover of the intestinal mucosa.6
Considering the literatures in the past were written before the introduction of newer small intestinal investigation modalities, the real incidence of small intestinal tumor may be higher than we had known. Recently we reported the overall frequency of small intestinal tumors as 4.3% in Korean national cohort of wireless capsule endoscopy (WCE) which was performed with indications including obscure gastrointestinal bleeding (OGIB), abdominal pain, weight loss, diarrhea, and so on.7 Similarly in a recent large scale European study, WCE revealed tumors in small bowel in 2.4%.8 This raises the possibility of increasing incidence of SB tumor in clinical practice with advance of new diagnostic technology.
THE CLINICAL PRESENTATIONS OF SMALL INTESTINAL TUMORS
The clinical manifestations of small intestinal tumors are generally vague and nonspecific. Nonspecific and vague symptoms include pain, nausea, and vomiting related to partial or complete bowel obstruction. Bleeding or perforation may occur.9,10 OGIB is the most common presentation of small intestinal tumors. In patients presenting OGIB, small intestinal tumors are diagnosed in around 6%.11-14 Weight loss, which occurs in approximately 30% to 50% of patients, should alert the physician to search for underlying organic causes and lead to a more thorough diagnostic workup, especially in patients aged over (older than) 50-years-old. Unexplained abdominal pain can also be the presentation of small intestinal tumors. In a Korean study, 2 out of 110 patients revealed small intestinal tumor as the causative lesion for unexplained abdominal pain in WCE evaluation.15 Because their clinical presentation is vague, a high index of suspicion is the key to diagnose them. Overt symptomatic tumors are often at advanced stage and have metastasis in a half of cases. Coupled with these undiscriminating presentations, the relative inaccessibility to the small bowel has been an obstacle in making a diagnosis. The majority of patients with small intestinal malignancies are diagnosed in the fifth or sixth decades of life. Patients with SB lymphomas are usually diagnosed a decade earlier.16 For all histologic types, and as with colorectal and gastric cancer, men tend to have a slightly higher rate of affliction than women.17,18
Genetically predisposing conditions such as familial adenomatous polyposis (FAP), hereditary non-polyposis colorectal cancer (HNPCC), celiac disease, and Peutz-Jeghers syndrome (PJS) are associated with increased incidence of the small intestinal adenocarcinoma (Table 1). Celiac disease is also associated with the enteropathy associated T-cell lymphoma in the small bowel. Personal history of colorectal cancer and Crohn's disease increase the possibility of development of small bowel adenocarcinoma. Acquired conditions including biliary diversion, ileostomy stomas, pouches, and conduits increase the risk of small bowel adenocarcinoma.5 It is also associated with the same carcinogens known to promote large bowel cancer such as a diet high in red meat, and alcohol and tobacco usage.19
Carcinoid tumor
Carcinoid tumor is the most common histological subtype in primary malignant small intestinal tumors, accounting for 20% to 50% of the total.2,16,20,21 The majority of small intestinal carcinoid tumors occur in the terminal ileum within 1 m from the ileocecal valve. Up to one third of patients have multiple tumors and patients with carcinoid tumors of the small bowel are at risk of a second gastrointestinal malignancy including gastric, colorectal, and pancreatic cancers.22 Because the majority of carcinoid tumors is small in size and grows very slowly, they are usually asymptomatic and are found incidentally during exploratory laparotomy or autopsy. Occasionally patients complain of episodes of abdominal pain consistent with intermittent bowel obstruction. When the primary carcinoid tumor reaches a size of 2 cm, the risk of metastasis to the liver increases substantially.21 With liver metastases there may be manifestations of the carcinoid syndrome, characterized by episodic flushing, watery diarrhea, and wheezing. Presence of the carcinoid syndrome simplifies diagnosis.
Carcinoid tumors of the small bowel are divided into two groups: tumors of the duodenum and upper jejunum and tumors of the distal jejunum and ileum. In the former group, gastrin-cell (G-cell) tumors predominate, followed by somatostatin-cell (D-cell) tumors, gangliocytic paraganglioma, and rarely, enterochromaffin-cell (EC-cell), serotonin-producing tumors. Conversely, endocrine tumors of the more distal segments of the small bowel are mostly EC-cell carcinoids.
Adenocarcinomas
Adenocarcinoma had historically been the most commonly diagnosed histological subtype of small intestinal tumors, but has recently been surpassed by carcinoid tumors according to the National Cancer Data Base.4 It accounts for approximately 33% of all primary malignant small bowel tumors.2,16,20,23 The small bowel adenocarcinoma was located 56% in duodenum, 16% in jejunum, and 13% in ileum. The exception to this presentation is seen in Crohn's disease, where the majority of adenocarcinoma occurs in the ileum. The proximal location of most small intestinal adenocarcinomas may reflect the presence of higher concentrations of bile, previously linked to increased risk for adenocarcinoma.24
Adenocarcinomas of the small bowel and colon are similar in many ways, including their development from adenomatous polyps and shared genetic susceptibility. Mutations in APC, K-ras, and p53 have all been demonstrated,25 but unlike colon cancer, APC mutations are not common. Molecular analysis of small intestinal adenocarcinoma has demonstrated the presence of high-microsatellite instability (MSI-H), associated with defects in DNA mismatch repair, in almost 20% of cases.26 Thus patients with small bowel adenocarcinomas are at increased risk of developing colorectal cancers and vice versa.27 Grossly, unlike ampullary and periampullary carcinomas, which are usually circumscribed and polypoid, small intestinal adenocarcinomas are usually large, annular, constricting, and centrally ulcerated masses with circumferential involvement of the intestinal wall. Regarding the anatomical distribution, duodenum is most frequently involved (55%) and followed by jejunum (30%) and ileum (15%).28 Microscopically, these tumors are very similar to their colonic counterparts, but with a higher proportion of poorly differentiated tumors. The prognosis of small intestinal adenocarcinoma is poor and the 5 year survival rate only remains at 25-30%.29,30
Primary gastrointestinal lymphomas
Small intestinal lymphoma constitutes 15-20% of all small intestinal neoplasms and 20-30% of all primary gastrointestinal lymphomas. Ileum is the most common site (60-65%) involved, followed by jejunum (20-25%), duodenum (6-8%) and other sites (8-9%).19 The clinical presentation of small intestinal lymphoma includes colicky abdominal pain, nausea, vomiting, weight loss and rarely acute obstructive symptoms, intussusceptions, perforation or diarrhea. Several types of lymphomas exist. Diffuse large B-cell lymphoma is most frequently observed. T-cell lymphoma and follicular lymphoma are more frequent in small intestinal cases than in gastric cases. Macroscopically, small intestinal lymphomas present as polypoid, ulcerative (including stricturing, non-stricturing and aneurysmal forms on radiography), multiple lymphomatous polyposis, diffuse, or other types.
Mesenchymal tumors
Mesenchymal tumors of the small bowel encompass a variety of benign and malignant tumors. With recent advances in immunohistochemistry, tumors lack of smooth muscle differentiation can be differentiated from leiomyoma and leiomyosarcoma. Spindle cell tumors arising from interstitial cells of Cajal, the cells that control intestinal motility, is nominated as GIST.31 GISTs are found most commonly in the stomach (approximately two thirds) followed by the small bowel (approximately one third).31 The size and shape varies in stomal tumors. Commonly, they are dome-shaped and submucosal with or without a central ulceration, or they may be large, fungating tumors that involve surrounding organs. Histologically, GISTs are essentially identical to their more frequent gastric counterparts, although epithelioid lesions are rather uncommon. GISTs are invariably immunoreactive for CD117 (KIT).31 Many GISTs have a demonstrable c-kit gene abnormality that can be therapeutically targeted using specific tyrosine kinase inhibitors. The factors predicting malignant GIST are size and mitotic or proliferative activity. In general, tumors over 5 cm in diameter and/or mitotic count greater than five mitoses per 50 high power field (HPF) are potentially malignant GIST. Smooth muscle neoplasms include leiomyoma and leiomyosarcoma. The smooth muscle phenotype must be immunohistochemically confirmed, as should the lack of CD117 (KIT) expression. Leiomyomas are usually small (<1 cm in diameter), well circumscribed, and submucosal lesions found incidentally and comprised of bland spindle cells showing low or moderate cellularity, mild or no cytologic atypia, and rare if any mitoses. However, leiomyosarcomas are generally larger tumors that may extend to involve adjacent structures and at times exhibit foci of hemorrhage or necrosis. Histologically, they can be distinguished from their benign counterpart by their increased cellularity, nuclear atypia, mitotic activity (usually >5/10 HPF), and tumor cell necrosis.
Melanoma
Intestinal melanomas can be primary tumors but metastases from cutaneous, ocular, or anal melanomas are more likely to happen.32,33 Metastatic lesions commonly involve jejunum and ileum and form multiple polypoid submucosal masses, less commonly as single mass. Masses are pigmented or amelanotic and the ulceration is commonly accompanied. The diagnosis of intestinal metastasis is often made far past to the early stage. A half of the patients with intestinal metastasis present extraintestinal metastasis at the time of diagnosis.34 Even after the curative surgical excision of primary cutaneous melanoma, intestinal metastasis is diagnosed after 6 months to 90 months.35,36 Enteroclysis is accepted as standard diagnostic method and positron emission tomography (PET) imaging can improve detection of melanoma metastases to the small bowel. However, radiologic modalities such as ultrasonography, upper gastrointestinal series (UGIS)/small bowel follow-through (SBFT), computed tomography (CT), PET yields over all detection rate of as low as 10-20%.37 Various treatment strategies have been tried in patients with intestinal melanoma, surgical removal of intestinal metastases is the treatment of choice in patients with resectable tumors. No systemic therapy improves survival in patients with melanoma metastatic to the bowel; thus, the prognosis for these patients is poor.
HOW TO DIAGNOSE SMALL INTESTINAL TUMOR
The diagnostic processes directed by the clinical presentation often start from the simplest examination modalities and findings are often vague and inconclusive. It has been usual that it takes 6 to 9 months to reach the final diagnosis.9,38 In advanced or complicated patients, simple abdominal radiography may reveal evidence of a small bowel obstruction or free air, prompting an exploratory laparotomy. Patients with the relatively chronic symptoms of abdominal pain, nausea, vomiting, weight loss, and signs of gastrointestinal bleeding have usually undergone an unrevealing workup including colonoscopy, esophagogastroduodenoscopy (EGD), and abdominal CT.
The UGIS/SBFT and enteroclysis
UGIS/SBFT remains the most commonly used method to examine the small bowel. It is relatively easy to carry out and makes easily tolerable discomfort to patients. UGIS/SBFT can detect the small intestinal ulcer, mass and intussusceptions but the sensitivity of small intestinal tumor diagnosis is usually around 30-44%.39 Especially for OGIB, the diagnostic yield reaches only 5%.
Conventional enteroclysis employing double contrast method showed better sensitivity for small intestinal disease and has been accepted as the diagnostic standard. For OGIB, the overall diagnostic yield of enteroclysis is around 10-20%. For small intestinal tumors, the sensitivity reached up to 90% in comparison to 33% of SBS/SBFT.40 However, enteroclysis has several fundamental limitations; it cannot visualize the luminal surface directly; it can miss the lesions of small size or lesions having continuous mucosal lining with adjacent mucosa; and it need highly skilled radiologist as well as makes significant discomfort to patient. In general, the contribution of enteroclysis to small intestinal tumor diagnosis occupies 50-60% only.41
CT
Though the advance of CT technology has allowed data acquisition over the entire abdomen in thin slices within one breath-hold, leading to fewer peristaltic and breathing artifacts, conventional CT scans detect only large size of intestinal tumors, at least over 1.0 cm in diameter. CT enteroclysis (CTE) is used to perform enhanced CT scanning and image post-processing after the small bowel is distended by administrating a high volume of contrast medium orally or via a nasojejunal catheter. It is easy to perform and produce reduced discomfort and less complication. The best merit for CTE lies in the fact that it not only provides the picture of the luminal side of mucosa but also provide the information about the changes in adjacent and related organs and structures. CTE can detect the mucosal changes, the cavitation or thickening of the wall, related lymph nodes status, mesentery, mesenteric vessels and the other organ structures. It helps us make an accurate pre-operative staging and design an appropriate treatment plan.42
In view of easy and safe procedure, CTE become the primary choice for the detection and localization of small intestinal tumors.43 One pro-study showed that CTE has a high sensitivity (100%) and specificity (95%) in the diagnosis of small intestinal diseases including tumors, Crohn's disease, small intestinal tuberculosis, small intestinal lymphoma associated with celiac disease, and intestinal obstruction.44 Regarding the size, CTE can detect tumors that are only 5 mm in diameter. The negative and positive predictive value of CTE for carcinoid tumor in patients with carcinoid symptoms were 100% and 94.7%, respectively.45
Magnetic resonance imaging (MRI)
MRI has the power to produce excellent soft tissue contrast and multiplanar imaging without radiation exposure. With the introduction of fast imaging techniques and improvement of contrast agents, MR enteroclysis (MRE) has been widely applied for the visualization of small intestinal diseases. It can not only be used to observe the mucous membrane but also reveals the pathological changes around the bowel. MRE can easily display small intestinal structures, especially in tumors with intestinal obstruction based on the signal difference generated by intestinal wall and luminal contrast agents. Recent study showed 95% of overall diagnostic accuracy for small intestinal tumors.46
Endoscopy
Gastroduodenal endoscopy is extremely accurate in identifying lesions proximal to the ligament of Treitz or in the terminal ileum. Push enteroscopes can reach and detect lesions located in the proximal jejunum, but not those in the mid to distal jejunum and ileum. Sonde enteroscopy, which is a 2,560 mm balloon-tipped endoscope, relies on small bowel peristalsis to propel the endoscope through the small bowel. Several studies reported that it is successful in visualizing up to 70% of the small bowel mucosa. The limitations of Sonde enteroscopy are need of expensive enteroscope, time consuming procedure up to 8 hours, and the inability to obtain biopsies.
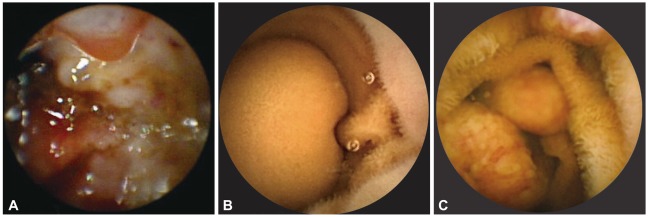
Two new endoscopic methods were introduced in 21st century. WCE travels along the small bowel and acquires over 50,000 images during 8-12 hour period. WCE can be performed in outpatient clinic and visualize the entire small bowel in a non-invasive manner (Fig. 1). Capsule retention may occur in points of pathology but not in normal condition.47 In general, the diagnostic yield of WCE in OGIB reaches up to 50-75%, higher in comparison with UGIS/SBFT and enteroclysis.48 In comparison with the push enteroscopy, WCE showed higher diagnostic yield (50-67.2% for WCE and 20-28% for push enteroscopy).49-51 In comparison with double balloon enteroscopy (DBE), the diagnostic yield of WCE was superior to that of DBE with one side approach and equivalent to that of DBE with both side approach.52 The detection rate of small intestinal tumors in WCE which is carried out for various kinds of indications is around 4%.7,8 Most common indication for WCE is OGIB. In comparison with other conventional radiologic studies, exclusive detection rate of small bowel tumor by WCE was reported as 52.6% (30 out of 57)7 to 65.2% (15 out of 23).53 However, WCE has also limitations. WCE moves passively by the intestinal peristalsis, WCE can miss the luminal lesion due to improper bowel preparation, presence of blood and rapid capsule transit. And tissue biopsy is not possible with WCE.
Balloon-assisted enteroscopy encompassing DBE and single balloon enteroscopy (SBE) was introduced in a decade ago. Like conventional endoscopies, DBE and SBE both allow direct and controlled visualization of the intestinal lumen. Regarding the range of examination, DBE and SBE can examine the whole length of the small bowel via both oral and anal approach. There are several factors which affect the completion of examination, including the procedure itself and the decision of operator. The overall completion of the small intestinal examination ranges 11.0-57.1%.54,55 The strength of DBE and SBE lies in the ability of tissue acquisition of lesion and simple therapeutic maneuvers such as clipping, polypectomy and cauterization are possible. In practice, the uses of DBE and SBE are confined to the conditions that suggest pathology in the small bowel and possibly need a therapeutic procedure. In a recent randomized controlled study, the overall diagnostic yield in various indications including OGIB reaches 50.0-61.1% and therapeutic outcomes reaches 27.8-35.0%.55 Regarding the detection of tumors in the small bowel, the small intestinal tumor or polyp were detected in 6-10%.55 In a Korean study, 13.8% of DBE procedures revealed small intestinal tumors regardless the indications for procedure12 and 7-20% in other literatures.11 In a study focusing on OGIB,56 the diagnostic yield was 45% and small intestinal tumor was detected in 13%. Among the patients with findings, 76% received endoscopic treatment.56 This is higher than that of WCE. It may result from the better control of visualization and patient selection difference. DBE can detect more small bowel tumors which are missed with WCE. In literature, among 18 small bowel tumors detected with DBE, the capsule identified lesions in only one third of the patients and missed all four cases of adenocarcinoma.57 Several studies have reported the usefulness of DBE in detecting and treating adenomatous polyps in the small bowel in patients at high risk such as FAP and PJS.58,59 The limitations of DBE are following; the complete small intestinal examination is not always possible; the discomfort, radiation exposure and possible complications are not negligible. Due to the limitations mentioned above, DBE or SBE as the first-line approach is not prudent in screening examination and elective diagnostic process. However, in patients at high risk and with proven tumors in WCE, DBE and SBE may offer better diagnostic yield and can provide therapeutic options.
Other modalities
There is no role for transcutaneous abdominal ultrasonography in the evaluation of patients with suspected small intestinal pathology except in pediatric patients with suspected intussusception, where the classic target sign can be seen. 111Indium octreotide imaging (octreotide scan) is a very useful technique when carcinoid tumor is suspected. The majority of carcinoid tumor cells express somatostatin receptors that bind the radio-labeled octreotide. Octreotide scanning has a 90% sensitivity rate for localizing carcinoid tumors in patients with the carcinoid syndrome and a 60% sensitivity rate in patients lacking the carcinoid syndrome.60
SURVEILLANCE OF THE SMALL INTESTINAL TUMORS FOR PATIENTS AT RISK
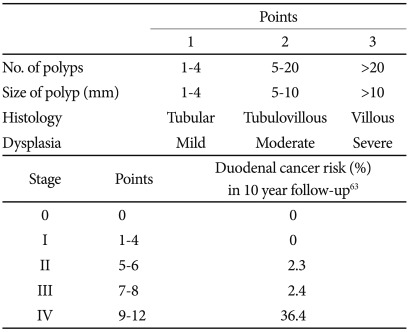
On the bases of known risk factors for small intestinal malignant tumors, patients at risk might have benefit from proper surveillance (Table 1). Patients with familial and nonfamilial polyposis syndrome are at increased risk of small intestinal cancer as well as colorectal cancer. The risk of small intestinal adenocarcinoma varies according to the types of polyposis syndrome. Not only adenomatous polyp, but hamartomatous polyps also have the foci of adenoma inside and these are associated with an increased risk of adenocarcinoma development. FAP is a well recognized condition in which adenomatous polyps develop in the region of the ampulla of Vater in 70-90% of patients, and 5-7% of adenomatous polyps undergo malignant change into adenocarcinoma.61 Predictors for cancer risk described by Spigelman et al.62 include the number, size, histology and degree of dysplasia (Table 2). In 10 year follow-up of duodenal polyps in FAP patients, Spigelman stage IV polyps developed into cancer in 36.4%.63 To reduce the risk of cancer from duodenal polyps, surveillance with duodenoscopy is recommended. In other site of the small bowel, jejunum and ileum, adenomatous polyps are detected in 75% of patients with FAP,64 but the cancer development has been rarely reported. Until now, there is no available data for usefulness of the small intestinal surveillance in FAP.
HNPCC is caused by germ line mutations of one of the mis-match repair genes, usually MLH1, MSH2, and MSH6. Affected individuals are highly susceptible to colorectal and endometrial cancer as well as small intestinal cancer. In 34-78% of patients, small intestinal cancer was the first malignant manifestation of HNPCC syndrome.65 For patients with HNPCC, the cumulative risk of small intestinal adenocarcinoma was estimated as 3-4% and it is more than 100 times the risk of the general population.65,66 This is similar to the lifetime risk of colorectal cancer in general population, and for which the screening surveillance is widely accepted as prudent. As a known risk factor, older aged population is more likely to have small intestinal adenocarcinoma. However, the patients with HNPCC present small intestinal adenocarcinoma 10-20 years earlier than the patients with sporadic small intestinal cancers which are diagnosed in sixth or seventh decades of life. And more than 10% of patients were diagnosed with small intestinal cancer before the age of 30 years.67 Male gender is slightly more affected than female. Localization in the small bowel is almost even in duodenum (45%), jejunum (29%), and ileum (12%).68 EGD surveillance in patients over 30 years old with HNPCC is recommended to detect both duodenal and gastric cancer which is also at increased risk in HNPCC.68 However, the rest of the small intestinal area cannot be examined with EGD. Regarding the small intestinal surveillance, we still need more evidence and consideration about cost/risk-benefit aspect. Early diagnosis and treatment of small intestinal adenoma/cancer in patients with HNPCC syndrome will probably improve prognosis. WCE can potentially detect these tumors in the presymptomatic stage, which is tentatively associated with better outcomes and several life-years possibly be gained. In a WCE study with 35 asymptomatic HNPCC patients, one adenocarcinoma and 2 adenomas were diagnosed.69
PJS is an inherited polyposis syndrome in which multiple characteristic polyps occur in the gastrointestinal tract, associated with mucocutaneous pigmentation, especially of the vermilion border of the lips. It is inherited in an autosomal dominant manner and is caused by a germline mutation in the STK11 (LKB1) gene. Polyps are found throughout the gastrointestinal tract but most are in the small bowel (60-90%) and colon (50-64%).70 Gastrointestinal polyps may cause gastrointestinal bleeding, anemia and abdominal pain due to intussusception, obstruction or infarction. Polyprelated symptoms usually arise in childhood and are seen by the age of 10 years in 33% and by 20 years in 50%. Regarding the cancer development in gastrointestinal tract, though it has been proposed that the hamartoma-adenoma-carcinoma pathway exists,71 the nature of carcinogenesis in PJS remains controversial. Based on epidemiologic and molecular genetic studies, it is widely accepted that there is increased risk of various cancers in PJS. Overall life time risk of any cancer reaches to 85-93% in PJS.72,73 Breast cancer (54%) and colon cancer (39%) are the most common cancers, followed by pancreatic cancer (36%).72 Life time incidence for the small bowel cancer is 1.7%73 to 13%.72 And the risk of cancer development increases rapidly after the age of 50.73 Though the consensus is not concrete, routine screening for upper gastrointestinal tract and colon is recommended, beginning at the age of 18, with 2-3 year interval.74-77 For small intestinal surveillance, the main indication is the prevention of intussusceptions and the need for emergency laparotomy. Though the data are limited, 68% of patients with PJS experience laparotomy by age of 18 and 30% at the age of 10.78 Recent proposal recommends small intestinal surveillance with WCE, beginning at the age of 18, with 3 year interval.74
And to prevent the need of intussusceptions laparotomy in childhood, additional baseline examination with WCE is also recommended at the age of 8. For this purpose, MRE and SBFT which show no difference in detection of polyp over 1.0 cm size can be reasonable alternatives.74
Patients with celiac disease have an increased risk for enteropathy-associated lymphomas as well as adenocarcinoma.79 Because the risk for both of these malignancies appears to be very small (<1%), there is no established role for surveillance endoscopy.80 However, the possibility should be considered in patients who have had celiac disease for many years. Those patients who become symptomatic after years of quiescent disease while strictly adhering to a gluten-free diet should be thoroughly investigated for a small intestinal malignancy.
Similarly, there is no established surveillance protocol for small intestinal cancer in patients with Crohn's disease. However, the development of a symptomatic small bowel stricture that does not respond to steroids should be suspected of harboring a malignancy and should be surgically resected.81 Also, presentation of patients with longstanding quiescent disease with small bowel obstruction suggests a newly developed small intestinal cancer.
In patients with cutaneous melanoma, intestinal metastasis is not uncommon condition and early detection of intestinal metastasis can possibly improve the chance of cure. Trial with WCE showed 20.4% detection rate of intestinal metastasis in cutaneous melanoma patients with intestinal blood loss and 28.6% in stage IV disease regardless of intestinal blood loss.82 Among those, a half of patients underwent intestinal surgery for metastasis. However, there are still limited data to evaluate the effect of WCE on the survival and a reasonable proposal to surveillance still doesn't exist.
CONCLUSIONS
Cancers arising in the small bowel pose a unique and difficult challenge to gastroenterologists, surgeons, and hematooncologists. The inaccessibility to the small bowel has now been overcome with newer CT/MR imaging and endoscopic modalities such as balloon assisted enteroscopy and capsule endoscopy. Newer diagnostic modalities provide clear and fine anatomical visualization of the small bowel and are approved to improve the diagnostic sensitivity and accuracy. Currently available data regarding the usefulness of new methods in diagnosis of small intestinal tumors are still limited, however, the prospective up to date are positive. With this recent diagnostic advance, the issues surrounding the screening and surveillance of small intestinal tumors in patient at risk should be assessed and the clinical outcomes of small intestinal tumors can possibly improve also.