INTRODUCTION
Fecaloma is a laminated mass of accumulated feces that is much harder in consistency than a fecal impaction.1 It is usually located in the sigmoid colon or rectum, but rarely in the cecum.2-4 Diagnosis is usually made from radiographic findings of a mobile intraluminal mass with a smooth outline and no mucosal attachment.2,5 Most fecalomas are successfully treated by conservative methods such as laxatives, enemas and rectal evacuation.2 When conservative treatments have failed, a surgical intervention may be needed.6 Only one case treated by an endoscopic procedure has recently been reported.7 We report here a case of cecal fecaloma, associated with an intestinal tuberculosis scar, that was successfully removed by endoscopic balloon dilatation of the stricture and mechanical destruction of the fecaloma with a polypectomy snare and grasping forceps.
CASE REPORT
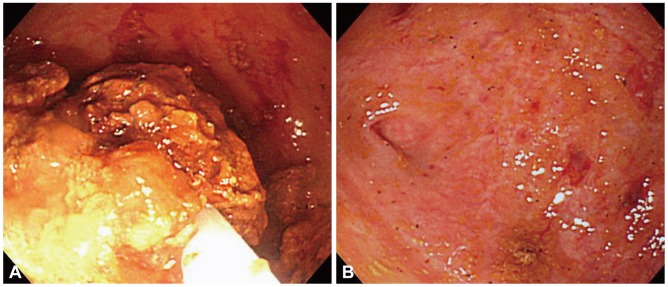
A 30-year-old female presented with a 2-month history of intermittent pain and a palpable mass in the right lower quadrant of the abdomen. She had a history of chronic constipation with about 2 bowel movements per week and hard stools. Five years earlier, she had undergone an appendectomy. She was diagnosed with pulmonary tuberculosis 9 months ago and was taking antituberculosis therapy. Her height was 163 cm and her weight was 49 kg. Physical examination revealed mild abdominal tenderness and a ping-pong ball-sized movable mass in the right lower quadrant of the abdomen. An abdominal computed tomography (CT) scan showed a 3.0-cm, round, laminated intraluminal mass with calcification in the cecum (Fig. 1A, B). Colonoscopy revealed fibrotic scar tissue probably due to intestinal tuberculosis in the ascending colon and a web-like stricture in the cecum around a patulous ileocecal valve. In a blind space which was formed by the stricture, a yellowish mass was found (Fig. 2). We could not insert a fiberoptic colonoscope into the cecum, and dilatation was thus performed using a th-rough-the-scope balloon (CRE balloon; Boston Scientific Co., Marlborough, MA, USA) with a diameter of 12 to 15 mm on inflation (Fig. 3). After endoscopic balloon dilatation, the colonoscope was able to pass into the cecum, and a 3.0-cm, yellowish fecaloma was observed. We broke down the fecaloma with a polypectomy snare and grasping forceps. The fecaloma was successfully removed by using a water jet and grasping forceps through the endoscopic procedure (Fig. 4A, B; Supplementary Video 1 online). There was no ulcer in the cecal base. Three mo-nths later, her symptoms improved, and there was no evidence of fecaloma recurrence.
DISCUSSION
Although fecal impaction is a common condition, fecaloma is an extremely rare form of impaction that refers to an accumulation of fecal material which forms a mass separable from the rest of the bowel contents.1 Fecaloma is found most frequently in the rectum or sigmoid because stools in the left colon become firmer and colon diameter is smaller on the left side than on the right side.6 The cecum is an unusual site, and only 4 cases have been reported in the English literature.2-4
There are several causes of fecaloma, and they have been described in patients suffering with chronic constipation, Hi-rschsprung's disease, Chagas' disease, and psychiatric diseases.8-10 It is thought that our case of fecaloma developed due to chronic constipation and prolonged impaction of fecal material in a pouch which was formed by stricture. This is the first case of fecaloma that was associated with an intestinal tuberculosis scar.
Diagnosis of fecaloma is usually made radiologically from a characteristic intraluminal mass seen on plain X-rays, barium enema and abdominal CT.2,5 The mass has smooth margins, some mobility within the bowel lumen and no attachment to the mucosal surface.
Complications of fecaloma are obstruction, ulceration, bleeding and perforation of the colon as well as hydronephrosis.11 Treatments include laxatives, enemas, rectal evacuation, surgical intervention and endoscopic removal.6 This is the second case of fecaloma that was removed successfully by the endoscopic procedure and the first case of cecal fecaloma that was removed successfully by the endoscopic procedure with endoscopic balloon dilatation.