Colonoscopic Cancer Surveillance in Inflammatory Bowel Disease: What's New Beyond Random Biopsy?
Article information
Abstract
Colonoscopy based colitis surveillance is widely accepted to try to prevent development of and ensure early detection of colitis-associated colorectal cancer. Traditionally this has been performed with quadrantic random biopsies throughout the colon. Chromoendoscopy "dye-spray" with targeted biopsies only has been shown to increase dysplasia detection 4 to 5 fold on a per lesion basis. It has therefore been suggested that random biopsies should be abandoned as they do not increase dysplasia detection nor change patient clinical course. Recent British guidelines for colitis surveillance have strongly endorsed chromoendoscopy. This short review summarizes current international guidelines and looks at how to optimize white light colonoscopy in colitis considering: bowel preparation, withdrawal time, high definition, and structure enhancement. Data for advanced imaging techniques are reviewed including positive evidence in favor of chromoendoscopy, and limited data suggesting autofluoresence imaging may be promising. Narrow band imaging does not increase dysplasia detection in colitis. Confocal endomicroscopy might potentially reduce biopsies beyond that of chromoendoscopy but does not offer a clear detection advantage. Pan-colonic chromoendoscopy with targeted biopsies increases dysplasia detection and is the standard of care in the United Kingdom. It is likely that the use of chromoendoscopy for colitis surveillance will become widely accepted internationally.
INTRODUCTION
Random biopsy, specifically quadrantic random biopsies taken every 10 cm throughout the colon during colonoscope withdrawal, has been a mainstay of colonoscopic inflammatory bowel disease (IBD) surveillance for the last 30 years. This arose from the premise that invisible so called "flat dysplasia in IBD" existed and was only detectable through histopathology. Random biopsy only samples 0.03% of the mucosal surface, has a detection rate of <2 per 1,000 biopsies and does not affect clinical decision making when advanced techniques are used.1,2 Although perhaps appropriate for its time when colonoscope optics were poorer (fibre optic or early video endoscopes) and colonoscopists were less familiar with the appearances of dysplasia in IBD, modern high definition (HD) instruments and adjunctive techniques make this now illogical as most dysplasia is or can be made visible. We have moved beyond random biopsy towards chromoendoscopy supported targeted biopsies only with endoscopic resection of circumscribed lesions. These two paradigm shifts in approach were recently specifically endorsed in the British Society of Gastroenterology (BSG) Guidelines 2010 for IBD surveillance3 as well as by the United Kingdom's National Institute for Clinical Excellence (NICE) Guidance 2011 (http://www.nice.org.uk/nicemedia/live/11877/48912/48912.pdf). NICE concluded that colonoscopic surveillance in IBD was cost effective for high risk groups, with an incremental cost effectiveness ratio (cost per quality adjusted life year) of £17,500 (US $27,150; ₩31,712,000). Nevertheless not all international guidelines have so far endorsed chromoendoscopy, summarized in Table 1.

Comparison of Screening Recommendation from International Guidelines for Patients with Colitis
WHEN TO PERFORM SURVEILLANCE
Colitis associated cancer risk increases with disease duration and disease extent. Surveillance is required for patients with both ulcerative colitis and Crohn's colitis as both are at increased risk. Previous British Guidelines recommended shorter surveillance intervals on the basis of disease duration as the risk was thought to increase exponentially to as much as 18% at 30 years;4 however more recent data from St. Mark's Hospital suggests risk may be linear and specific risk factors may be more important (Table 2). Risk in population based cohorts seems lower than from specialist centers. This has lead to the concept of risk stratified surveillance where those at highest risk e.g., with primary sclerosing cholangitis or previous dysplasia receive short surveillance intervals of 1 year, whist those at lowest risk e.g., left sided colitis without inflammation have longer surveillance intervals of 5 years. This risk based stratification is used in British Guidelines, and in part by European Crohn's and Colitis Organization (ECCO) guidance. The combination of risk based surveillance and chromoendoscopy without targeted biopsies may be cost saving.5
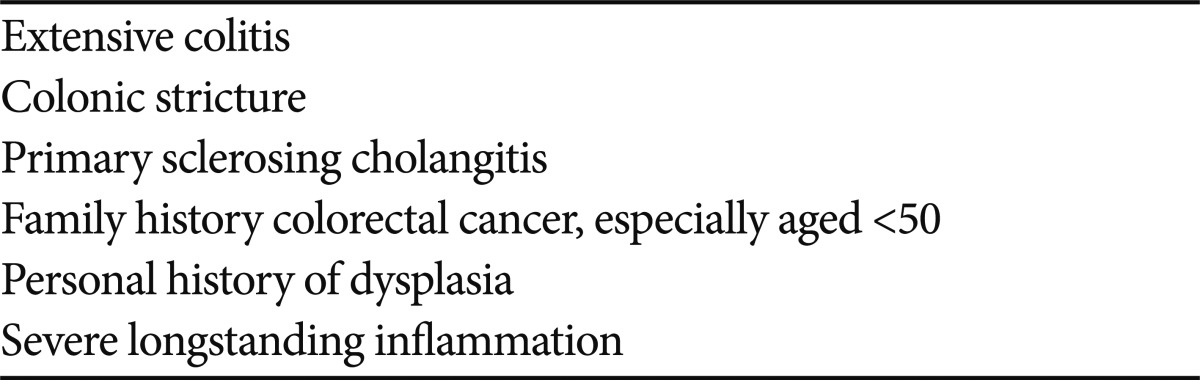
Risk Factors for Dysplasia in Ulcerative Colitis
BETTER WHITE LIGHT ENDOSCOPY
Bowel preparation and clinical remission
We know that we need good bowel preparation to find polyps in non-colitic colonoscopy,6 and we also know that bowel preparation is worse in colitis, odds ratio 0.63 (95% confidence interval [CI], 0.40 to 0.98).7 The lack of research into bowel preparation in colitis is therefore puzzling, particularly for a patient group who need to have a good experience with bowel preparation for repeated examinations. Good quality prep in colitis is likely to improve detection rates, and is essential before trying to apply adjunctive techniques such as chromoendoscopy or other advanced imaging techniques. Similarly examination in clinical remission is critical to have a reasonable chance of detecting dysplasia, as detection of flat lesions against an inflamed background is much more difficult. Anecdotally patients not in remission also tend to prepare less well.
Withdrawal time
Taking longer for withdrawal has been clearly shown to be associated with improved adenoma detection in non-colitis patients. Logically this should also apply in colitis where detection is even more difficult. Toruner et al.8 were able to demonstrate this is a retrospective analysis looking at median procedure duration versus dysplasia detection rate and showed a significant association between longer procedure duration and increased dysplasia detection (R2=0.12; p=0.0066).
HD and structure enhancement (SE)
All major endoscope manufacturers offer HD instruments, with an option for push button digital image SE. This latter function helps improve edge definition, a critical element in detecting lesions in colitis. It is logical therefore to select the instrument with the best resolution and apply available SE to optimize white light endoscopy when performing colitis surveillance, though formal supportive data is lacking.
NEW TECHNOLOGY AND TECHNIQUES
Chromoendoscopy
There have been at least five of studies that have looked at the efficacy of chromoendoscopy for colitis surveillance utilizing randomized, back-to-back, and case-control designs (Table 3).9-13 All have been positive in favor of chromoendoscopy with a per patient increase in dysplasia of approximately 2 to 3 fold and a per lesion increase of 4 to 5 fold. Studies have used both methylene blue and indigo carmine. Given the consistent evidence in favor of chromoendoscopy BSG guidelines in 2010 strongly endorsed chromoendoscopy with targeted biopsies of circumscribed lesions but without random biopsies. ECCO Guidelines give more qualified support. Kiesslich and Neurath14 give a helpful summary of how to optimize chromoscopic technique in their SURFACE guidelines. Although more time consuming than white light endoscopy alone, an extra 10 to 15 minutes, the time is probably equivalent to white light examination with 32 or more biopsies.

Summary of Trials Comparing White Light and Chromoendoscopy Dysplasia Detection for Colitis Surveillance on a per Patient Basis
Narrow band imaging (NBI) and autofluorescence
There was great hope that NBI would be able to act as a form of "electronic chromoendoscopy" to make colitis surveillance more efficient. Unfortunately, probably due to the background inflammation, dysplasia detection was no different to white light in two tandem studies and one multi-centre, randomized, parallel group study (Table 4).15-17 It seems unlikely that NBI will be helpful for dysplasia detection in colitis. Autofluorescence imaging (AFI) has had more success with a case report suggesting that 50% of AFI positive lesions were dysplastic. A small (n=50) back-to-back study showed a lower miss rate with AFI than white light (0/10 vs. 3/6, p=0.036).18 Anecdotally inflammation is a problem.

Outcomes of Studies Comparing NBI and WLE for Dysplasia Detection in Colitis
Confocal endomicroscopy
Confocal endomicroscopy has been proposed as an addition to chromoscopically detected lesions to help target biopsies and reduce their number. In a study by Kiesslich et al.,11 chromoendoscopy reduced biopsies 10-fold. Addition of confocal could have reduced the number of biopsies a further 5-fold to approximately 1 per patient.11 Although there is the potential to have to take very few biopsies, the technique is technically demanding and the instruments currently unwieldy and not HD. Given two expert pathologists are required to make a clear diagnosis of dysplasia in IBD, the challenge for a single endoscopist to do this in vivo is considerable. Definite advantages of this approach are not yet conclusively demonstrated.
CONCLUSIONS
Pan-colonic chromoendoscopy without random biopsies is now the standard of care in the United Kingdom for colonoscopic colitis surveillance and is likely to be adopted more widely. This will lead to increased dysplasia detection. Other technologies are not yet proven, though AFI has some promise. Strategies where endoscopically resected polypoid dysplasia in colitis leads to further surveillance rather then colectomy will need to be considered.
Notes
The author has no financial conflicts of interest.