Kang and Hyun: Preparation and Patient Evaluation for Safe Gastrointestinal Endoscopy
Abstract
Patient evaluation and preparation is the first and mandatory step to ensure safety and quality of endoscopic procedures. This begins and ends with identifying the patient, procedure type, and indication. Every patient has the right to be fully informed about risks and benefits of what is to be performed on them, and the medical personnel should respect the decision made by the patients. Thoroughly performed history taking and physical examination will guide the endoscopists to better stratify risk and plan sedation. Special attention should be given to higher-risk patients with higher-risk condition undergoing higher-risk procedures. Making preparations to monitor the patients and being ready to handle emergency situations throughout the endoscopic procedure are sine qua non to warrant safe endoscopy.
Keywords: Preparation; Patient evaluation; Safety; Endoscopy
INTRODUCTION
Gastrointestinal (GI) endoscopy allows direct visualization of the interior of the GI tract and is frequently performed to investigate symptoms, confirm diagnosis, and offer treatment. In the past, the realm of GI tract for endoscopists has chiefly been limited to the upper and lower GI tract, and the small bowel has largely been considered a "no man's land" until the advent of enteroscopy. However, with the enteroscope at hand, examination of the entire GI tract has become possible. In addition, the introduction of endoscopic retrograde cholangiopancreatography (ERCP) has provided endoscopists with an invaluable tool to evaluate and manage diverse problems of the biliary and pancreatic ductal systems. Furthermore, endoscopic ultrasonography (EUS) has granted access to organs and lesions in the vicinity of the GI tract. 1 Along with the expansion of the realm of endoscopic procedures, the possibility of the occurrence of complications has also increased. Therefore, more precaution should be taken regarding its safety. Since many endoscopic procedures are performed under sedation/analgesia nowadays, safety regarding sedation should be considered as well. There are many factors that need to be taken into account in order to perform safe endoscopy. Although each endoscopic procedure has its own necessary preparation and precautions, many are common to all and can be divided into three procedural steps: preprocedure, intraprocedure, and postprocedure. The components of preprocedural preparation essential for safe endoscopy are as follows:
Identification of patient, procedure type, and indication Informed consent History taking and physical examination Risk stratification and sedation planning Antibiotic prophylaxis Antithrombotics: anticoagulants and antiplatelet agents Patient monitoring devices Preparation for emergency situations Time-out
This article will focus on patient evaluation and preparation that are necessary up to the point before the actual endoscopic examination is initiated, i.e., prior to sedative administration or scope insertion.
PREPARATION AND PATIENT EVALUATION
Identification of patient, procedure type, and indication
Identifying the patient is the first step that should be undertaken when a patient arrives at the endoscopy unit. Patient identification can be done using hospital registration number, name, social security number, date of birth, etc. One of the most common ways to identify the patient is by matching the name. When doing so, one should ask open-ended questions, e.g., "What is your name?" instead of pronouncing the patient's name on the chart and ask if it is correct. Since there can be patients with the same name, it is not sufficient to identify the patient with name alone. Therefore, it is generally recommended that the patient be identified by confirming at least two of the patient data which should preferably be asked in an open-ended manner whenever possible. In case communication with the patient is not possible because the patient is unable to speak or is a foreigner, checking photo identification card could be an option.
Once it has been identified that the right patient has arrived, the type (esophagogastroduodenoscopy, colonoscopy, flexible sigmoidoscopy, enteroscopy, EUS, or ERCP) and indication of endoscopic procedure the patient is to undergo should be verified. The indications for endoscopic examination can be for screening, surveillance, diagnostic (especially for symptom evaluation) or therapeutic purposes. Although ordering endoscopic examination is largely at the discretion of the physicians, indications for endoscopy should be appropriate and acceptable so as to be beneficial to the patients by having an impact on clinical decision making or outcome. 2 Since the type of endoscopic procedure mainly depends on its indication, being familiar with the indication for that patient will help the endoscopy team to make pertinent preparations and take necessary precautions specific to that procedure.
Informed consent
Informed consent in endoscopy can be defined as "voluntary agreement by a patient with sound decision making capacity to undergo proposed endoscopic procedure after adequately understanding the purpose, nature, benefit, risks, complications, and alternatives related to the procedure." 3, 4 Thus, informed consent is not merely signing the consent form at the end of the document but a process that is both ethically and legally important. Properly obtained informed consent would serve to uphold the right of the patient and protect the physicians from malpractice litigation. Although the contents of the informed consent would vary depending on the proposed procedures, it is recommendable to disclose the following elements for all endoscopic procedures: 4
Medical diagnosis Procedure name Purpose and necessity of the procedure Nature and procedural steps of the proposed procedure Anticipated benefits and expected outcomes of the procedure Necessary precautions before and after the procedure Potential risks and possible complications of the procedure Reasonable alternatives to the procedure Prognosis and outcome if the procedure is not performed Date, time, name, and signature legibly written by patient and physician
Enough and relevant information on each of the above elements should be given to and understood by the patient. For that purpose, informed consent should be obtained by medical personnel, preferably by those directly involved with the procedure. The procedural steps should be sufficiently outlined and success rate of the procedure should be given. When explaining the risks and complications related to the procedure, the relative incidence and the gravity should be detailed. It is generally not necessary to list every potential risks and possible complications. However, those with significant frequency and those that could affect patient's decision on whether or not to undergo the procedure should not be left out. When presenting the reasonable alternatives, all possible options should be disclosed even the ones that could carry higher risk compared to the proposed procedure.
Informed consent should be obtained prior to every endoscopic procedure, be it for diagnostic or therapeutic purposes. If the patient is to undergo endoscopy under sedation, informed consent should also be obtained for sedation. Informed consent can be obtained by writing and explaining the aforementioned information on a piece of paper, but it is more common and advisable to use a preprinted form so as not to leave out any pertinent information. In both cases, it should be written in simple language that is understandable to patients who in most instances are nonmedical personnel.
Before signing the document, the patient should be given enough time to ask questions and discuss face to face with the medical personnel obtaining the informed consent. When the patient agrees to undergo the proposed procedure, the document should be legibly dated, timed, named, and signed both by the physician and the patient at the end of each informed consent at free will. If the patient is a minor, incompetent or incapacitated, the informed consent should be signed by parents, legal guardian, or surrogate of the patient. Involving a third party to witness the informed consent process would be a wise option if problem is deemed to arise regarding its legality.
History taking and physical examination
Although history taking and physical examination is important both for patients undergoing endoscopic procedures with no sedation or with sedation/analgesia, it is especially important if moderate or deep sedation is planned. In these patients, sedation-oriented medical history should be obtained and sedation-directed physical examination should be performed. The following is a list of sedation-oriented medical history recommended by American Society of Anesthesiologists (ASA): 5
Abnormalities of the major organ systems Previous adverse experience with sedation/analgesia as well as regional and general anesthesia Drug allergies, current medications, and potential drug interactions Time and nature of last oral intake History of tobacco, alcohol, or substance use or abuse
Patient's medical history should be thoroughly reviewed for the presence of significant cardiovascular (heart failure, angina pectoris, myocardial infarction, arrhythmia), respiratory (asthma, chronic obstructive pulmonary disease, sleep apnea, snoring), neurologic (seizure, stroke), psychiatric, endocrine (diabetes mellitus), and renal (end-stage renal disease) problems. History on prior surgery of GI tract that could affect the endoscopic procedure should also be asked. Previous adverse experience to sedation/analgesia and anesthesia need to be documented. Although debate still exists, precaution must be taken when using propofol since there have been reports that allergic reaction could occur after propofol administration in individuals with egg allergy. 6 Bleeding tendency should be noted and coagulation profiles checked when necessary. The time from last oral intake (fluid or solid food) should be recorded. Recommended minimum fasting period ranges from 2 hours for clear liquids to 6 hours for light meal. 7 Since fatty food or meal that includes meat may prolong gastric emptying time, fasting for at least 8 hours is domestically recommended. History on substance use or abuse is also very important. Since narcotics, such as fentanyl patch and morphine, can potentiate the action of sedatives and analgesics, care must be taken in determining the dose necessary for sedation. On the other hand, adequate sedation may not be achieved with standard amount of sedatives in patients taking benzodiazepine or neuropsychiatric medications. Augmented dose of sedatives is also usually required for those with a history of alcohol abuse. All women of childbearing age should be questioned regarding the possibility of pregnancy. Patients with cardiac pacemaker or defibrillator should not be overlooked since certain endoscopic procedures demand special attention. Physical examination should be directed towards positive medical history. The essential components that should be included are as follows:
Vital signs and weight Auscultation of the heart and lungs Baseline level of consciousness Assessment of airway
Blood pressure, body temperature, pulse rate, and respiratory rate should be checked and recorded before endoscopic procedure in every patient. If the patient is to undergo endoscopy under sedation, body weight should also be measured to calculate the amount of sedatives and analgesia to be administered. It is advisable to auscultate the heart and lungs (wheezing or stridor) prior to the procedure, especially for those with cardiovascular and respiratory problems. Assessing the components of airway anatomy is crucial if sedation/analgesia is planned: significant obesity, short neck, limited neck motion, micro/retrognathia, limited mouth opening, craniofacial anomaly, denture, loose teeth, etc.
Risk stratification and sedation plan
Presently, there is no stratification system specifically devised for sedative endoscopy that can be used to assess comorbidity and to predict periprocedural morbidity and mortality. The most commonly adopted risk stratification system is the ASA physical status classification. Since its introduction in 1941, 8 it has undergone several modifications and amendments to assume the current version of ASA physical status classification shown in Table 1. 9- 11 There are several limitations to this stratification system. To begin with, it does not provide specific examples for each class or present additional information to further define these categories. Therefore, different endoscopists and anesthesiologists may assign different physical status classes to the same patient, thus being prone to interobserver variability. In addition, this classification does not take age or presence of malignancy into consideration which could be important factors influencing patients' general physical status. Moreover, physical status can exist that does not fall into a specific class but exist somewhere in between. Despite these drawbacks, several studies have shown that high ASA physical status classification correlated with increased risk of adverse events. 12- 14 Therefore, it seems reasonable to use this system for stratifying periprocedural risks related to the endoscopic procedure. Nevertheless, endoscopists are best advised not to rely solely on this system but to consider it as one of the components of overall procedural risk assessment. If the patient is to undergo endoscopic procedure under sedation/analgesia, the intended level of sedation should be planned: minimal sedation (anxiolysis), moderate sedation/analgesia (conscious sedation), deep sedation/analgesia, and general anesthesia. 5 Moderate sedation/analgesia is sufficient for most endoscopic procedures, but deeper sedation/analgesia could be necessary for procedures that take longer, such as ERCP, EUS┬▒fine needle aspiration (FNA), and endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD).
Antibiotic prophylaxis
Bacteremia has been shown to occur during almost all endoscopic procedures, but in most instances antibiotics prophylaxis is generally not recommended. The rationale for this is based on the fact that bacteremia also occurs during routine daily activity (brushing and flossing of teeth, use of toothpicks, and even chewing food) which are largely transient and innocuous. However, antibiotic prophylaxis is necessary in a subset of patient condition and/or for certain procedures as recommended by the American Society for Gastrointestinal Endoscopy (ASGE) in 2008. 15 Periprocedural antibiotic prophylaxis in this subset of patients is intended to reduce risk of local and systemic infection related to endoscopic procedure. It is worth noting that antibiotic prophylaxis before endoscopic procedures only to prevent infective endocarditis is currently not recommended based on the revised guideline by the American Heart Association/American College of Cardiology. 16
In short, antibiotic prophylaxis is necessary in high-risk patients and for high-risk procedures as listed below.
-
High-risk patients needing antibiotic prophylaxis
Cirrhosis and acute GI bleeding Pancreatic fluid collection communicating with pancreatic duct (only for ERCP and transmural drainage)
-
High-risk procedures needing antibiotic prophylaxis
Transmural drainage for sterile pancreatic fluid collection EUS-FNA for cystic lesions along GI tract ERCP to relieve obstructed bile duct in patients without cholangitis (when incomplete drainage anticipated) Percutaneous endoscopic gastrostomy (PEG) Natural orifice transluminal endoscopic surgery (NOTES)
All cirrhosis patients who present with acute GI bleeding should receive prophylactic antibiotic therapy at admission regardless of endoscopic procedure. Patients with sterile pancreatic fluid collection-pancreatic cysts (including pseudocysts) or necrosis-that is connected to the pancreatic duct can be considered as high-risk patients needing antibiotic prophylaxis only if they are to undergo ERCP or transmural drainage. If there is no connection between the pancreatic fluid and pancreatic duct, ERCP poses no risk; but transmural drainage in this case does pose a risk for cyst infection and thus should be considered high-risk procedure needing antibiotic prophylaxis. In lieu of transmural drainage, EUS-FNA is being widely performed for both cystic and solid lesions. Endoscopists should not forget to administer antibiotics prior to performing EUS-FNA for cystic lesions anywhere in the GI tract, including the mediastinum. When a patient presents with obstructive cholangitis, antibiotics should be instituted immediately. However, antibiotic administration is not recommended before ERCP if the patient has bile duct obstruction but not cholangitis. Nevertheless, if it is deemed that ERCP cannot completely resolve the obstruction, as is often the case with hilar strictures and primary sclerosing cholangitis, prophylactic antibiotics should be given. There is no debate regarding the necessity of administering antibiotics to all patients undergoing PEG to prevent skin infection, preferably 30 minutes before the procedure. As for NOTES, there are insufficient data to make recommendations on antibiotic prophylaxis, but is generally viewed as beneficial considering the invasive nature of the procedure. 17
Antithrombotics: anticoagulants and antiplatelet agents
Antithrombotic agents are widely prescribed nowadays for primary and secondary cardiovascular prevention. They can be divided as follows:
-
Anticoagulants
Warfarin Heparin Low molecular weight heparin
-
Antiplatelet agents
Aspirin Nonsteroidal anti-inflammatory drugs Thienopyridines (clopidogrel and ticlopidine) Glycoprotein IIb/IIIa receptor inhibitors
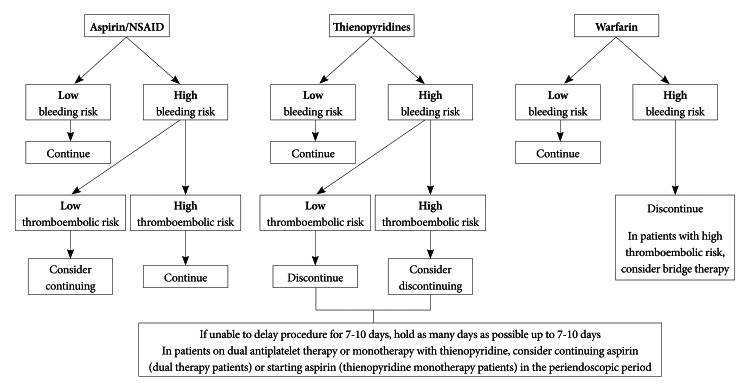
Occasionally, patients on antithrombotic agents need to undergo endoscopic procedures. In these situations, it is crucial to evaluate whether antithrombotic agents can or should be withheld before the procedure. To do so, it is fist necessary to take three factors into account: type of antithrombotic agents being used, procedure risk for bleeding (low-risk procedure/higher-risk procedure) ( Table 2), and condition risk for thromboembolic event (low-risk condition/higher-risk condition) ( Table 3). The two most frequently consulted guidelines on the management of antithrombotic agents for endoscopic procedures are the ones issued by British Society of Gastroenterology in 2008 and ASGE in 2009. 18, 19 Although the algorithm for decision making is a little different, both guidelines are based on the aforementioned three factors ( Fig. 1). In short, all antithrombotic agents are suggested to be continued for low-risk procedures. Aspirin/NSAIDs need not be discontinued regardless of condition risk for thromboembolic event. However, in patients taking thienopyridines and warfarin, situations vary for higher-risk procedures depending on the condition risk of thromboembolic event. For higher-risk procedure in patients with low-risk condition, thienopyridines is recommended to be discontinued for 7 to 10 days and aspirin maintained or substituted. Warfarin should be stopped for 3 to 5 days and no bridge therapy is necessary in these patients. For higher-risk procedure in patients with higher-risk condition, it is preferable to delay the procedure and continue using thienopyridines until its minimum recommended duration has been sufficed (e.g., >12 months after the insertion of drug eluting coronary stent, >1 month after the insertion of bare metal coronary stent). However, if the procedure cannot wait, aspirin should be maintained or substituted. As for warfarin, it needs to be discontinued for 3 to 5 days before the procedure and bridge should be considered. It is interesting to note that the practice pattern on the management of antithrombotic agents somewhat differ between Eastern and Western endoscopists depending on where the emphasis is, i.e., bleeding risk or thromboembolic risk. 20, 21
Patient monitoring devices
Most endoscopic procedures can be adequately performed with the patient under moderate sedation, which is also commonly referred to as "conscious sedation." However, more complex procedures that require prolonged procedure time may need to resort to deep sedation. If a patient is to undergo endoscopic procedures with moderate or deep sedation, patient status should be monitored accordingly. 5, 22
The standard parameters of patient status that need to be periodically checked before, during, and after the procedure include blood pressure, oxygen saturation, pulse rate (heart rate), and level of consciousness. Blood pressure is generally measured noninvasively with blood pressure cuffs. Oxygen saturation can be monitored with pulse oximeter to detect oxygen desaturation and hypoxemia. However, if prolonged procedure time is anticipated as is the case with ERCP, EUS┬▒FNA, and EMR/ESD, capnography may prove to be of more benefit in measuring respiratory activity. 21 Oxygen supplementation is recommended for both moderate and deep sedation to reduce the degree of oxygen desaturation. Pulse rate is normally monitored using pulse oximeter, which is generally sufficient for the majority of endoscopic procedures. However, electrocardiogram monitoring may be beneficial when the procedure time is expected to be prolonged; it is also recommended for patient with significant cardiopulmonary disease, arrhythmia, and advanced age. Level of consciousness should be monitored directly by evaluating the patient.
Preparation for emergency situations
Emergency situations that are related to sedation or procedure can arise throughout endoscopy. Therefore, the endoscopy team should always be prepared to cope with these situations. It is mandatory for all members of the team to periodically receive education and be currently certified in basic life support. At least one member of the team should have current certification on advanced cardiac life support. All equipment and medications necessary to perform emergency resuscitation should be available at any time during endoscopic procedure. Adequate accessories and devices (injector, coagulator, hemoclips, etc.) also should be prepared to manage procedure related complication such as bleeding and perforation. 23, 24
Time-out
Before inserting the endoscope or administering sedatives, the endoscopy team should gather together and perform "time-out" or "team pause" to verify that correct indicated procedure is to be performed on the right patient with appropriate apparatus. It should be emphasized that, as mentioned before, patient should be confirmed by using at least two of the identifiable parameters. When time-out has been carried out, the patient is now ready to undergo endoscopic procedure. If the endoscopist, endoscopy nurses, and assistants have washed their hands before the procedure and put on their protective gown and gloves, the endoscopy team is also ready to begin the exam.
CONCLUSIONS
Introduction of GI endoscopy has revolutionized the diagnosis and management of diseases of the GI tract. Further advances in endoscopy have empowered the endoscopists to explore not only the entire GI tract but also its vicinity. In addition, adoption of sedation to endoscopy has conferred comfort to the patients undergoing the procedure. These progresses have no doubt brought many benefits both to the endoscopists and the patients, but not without costs. As the frontier of endoscopic procedures expanded and the use of sedation became widespread, the likelihood of the occurrence of adverse events also increased. Therefore, it is imperative for medical personnel to be fully aware of the necessary preparations/precautions and carry them out accordingly in order to perform safe endoscopy. Medical personnel should also be capacitated to be able to manage diverse medical emergencies that could arise during the endoscopic procedures. Conforming to these safety measures is indispensable for assuring high-quality endoscopy, and this will help the endoscopists to ach-ieve the ultimate goal which is to provide patients with the best possible care.
References
2. American Society for Gastrointestinal Endoscopy. Appropriate use of gastrointestinal endoscopy. Gastrointest Endosc 2000;52:831ŌĆō837.  3. Pape T. Legal and ethical considerations of informed consent. AORN J 1997;65:1122ŌĆō1127. 9187459.  4. Standards of Practice Committee. Zuckerman MJ, Shen B, et al. Informed consent for GI endoscopy. Gastrointest Endosc 2007;66:213ŌĆō218. 17643691. 6. Training Committee. American Society for Gastrointestinal Endoscopy. Training guideline for use of propofol in gastrointestinal endoscopy. Gastrointest Endosc 2004;60:167ŌĆō172. 15278039. 7. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures: a report by the American Society of Anesthesiologist Task Force on Preoperative Fasting. Anesthesiology 1999;90:896ŌĆō905. 10078693. 8. Saklad M. Grading of patients for surgical procedures. Anesthesiology 1941;2:281ŌĆō284. 9. Dripps RD, Lamont A, Eckenhoff JE. The role of anesthesia in surgical mortality. JAMA 1961;178:261ŌĆō266. 13887881. 10. Fitz-Henry J. The ASA classification and peri-operative risk. Ann R Coll Surg Engl 2011;93:185ŌĆō187. 21477427. 11. American Society of Anesthesiologists. American Society of Anesthesiologists physical status classification [Internet]. Park Ridge: American Society of Anesthesiologists; c1995. cited 2013 Feb 20]. Available from: http://www.asahq.org. 12. Sharma VK, Nguyen CC, Crowell MD, Lieberman DA, de Garmo P, Fleischer DE. A national study of cardiopulmonary unplanned events after GI endoscopy. Gastrointest Endosc 2007;66:27ŌĆō34. 17591470. 14. Vargo JJ, Holub JL, Faigel DO, Lieberman DA, Eisen GM. Risk factors for cardiopulmonary events during propofol-mediated upper endoscopy and colonoscopy. Aliment Pharmacol Ther 2006;24:955ŌĆō963. 16948807. 15. ASGE Standards of Practice Committee. Banerjee S, Shen B, et al. Antibiotic prophylaxis for GI endoscopy. Gastrointest Endosc 2008;67:791ŌĆō798. 18374919. 16. Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation 2007;116:1736ŌĆō1754. 17446442. 18. Veitch AM, Baglin TP, Gershlick AH, Harnden SM, Tighe R, Cairns S. Guidelines for the management of anticoagulant and antiplatelet therapy in patients undergoing endoscopic procedures. Gut 2008;57:1322ŌĆō1329. 18469092. 19. ASGE Standards of Practice Committee. Anderson MA, Ben-Menachem T, et al. Management of antithrombotic agents for endoscopic procedures. Gastrointest Endosc 2009;70:1060ŌĆō1070. 19889407. 20. Lee SY, Tang SJ, Rockey DC, et al. Managing anticoagulation and antiplatelet medications in GI endoscopy: a survey comparing the East and the West. Gastrointest Endosc 2008;67:1076ŌĆō1081. 18384789. 22. Standards of Practice Committee of the American Society for Gastrointestinal Endoscopy. Lichtenstein DR, Jagannath S, et al. Sedation and anesthesia in GI endoscopy. Gastrointest Endosc 2008;68:815ŌĆō826. 18984096.
Fig.┬Ā1
Management of antithrombotic agents in the elective endoscopic setting. Adapted from ASGE Standards of Practice Committee et al. Gastrointest Endosc 2009;70:1060-1070, with permission from Elsevier. 18
Table┬Ā1
American Society of Anesthesiologists Physical Status Classification 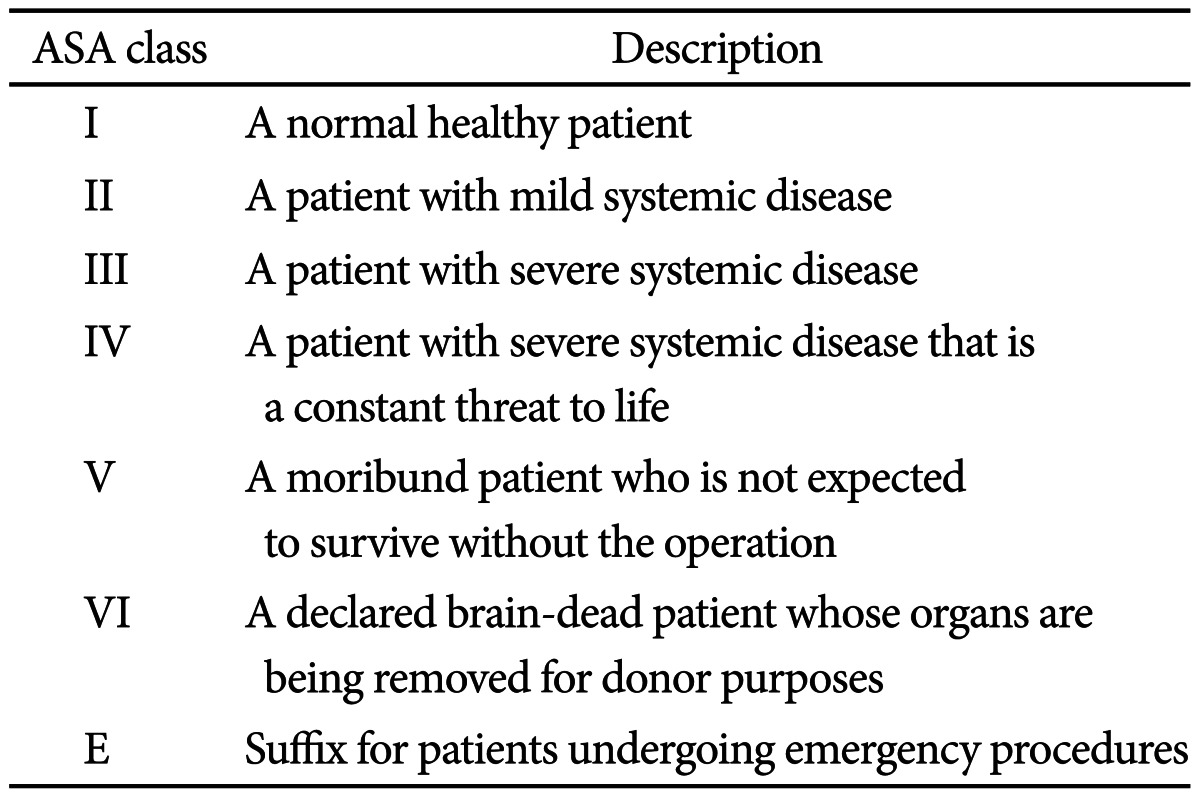
Table┬Ā2
Procedure Risk for Bleeding 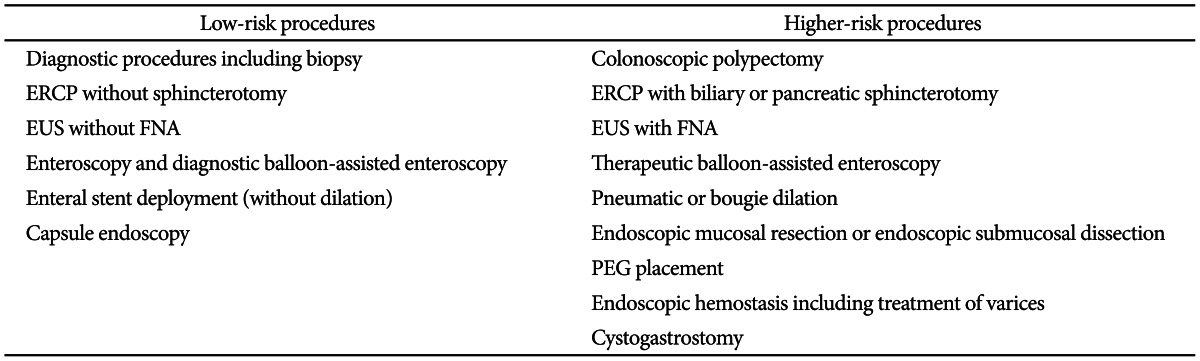
Table┬Ā3
Condition Risk for Thromboembolic Event 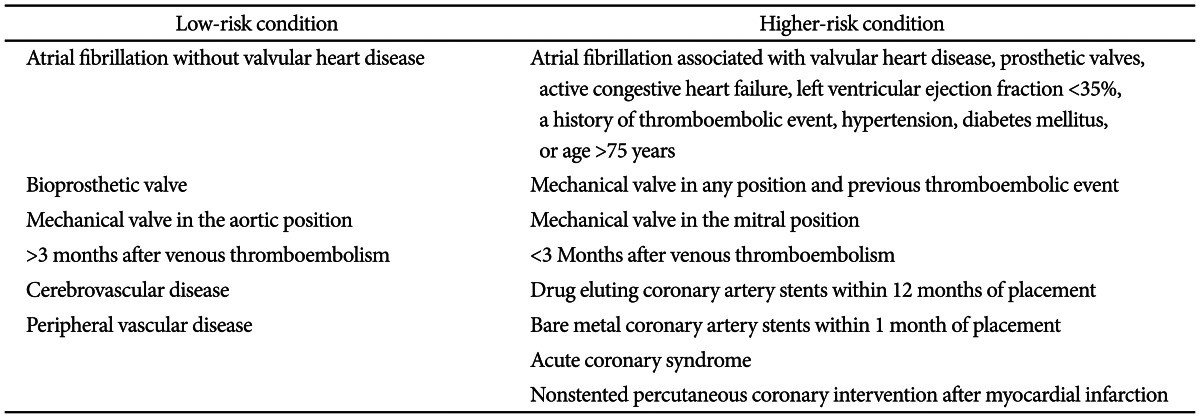
|
|





