INTRODUCTION
Endoscopic placement of biliary stent is an effective treatment for benign biliary stricture. Recently, a covered self-expandable metal stent (SEMS) is being used. The advantages of the covered SEMS is prolonged patency, lower failure, few complications, and more easiness in its removal.1 However, a rare complication of stent fracture is reported due to the possibility of metal fatigue, tearing of polyurethane stent cover, or application of laser, electrocoagulation.2 Proximal or distal migration is another complication after stent insertion. So far, just a few cases of proximal migration of SEMS have been reported. This report describes that the complication of SEMS fracture during endoscopic retrieval of the stent and proximal migration of the remnant stent in patient with chronic pancreatitis.
CASE REPORT
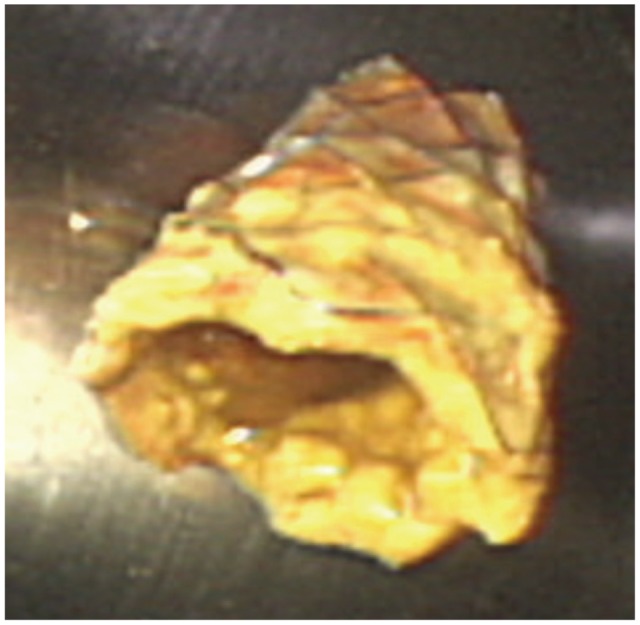
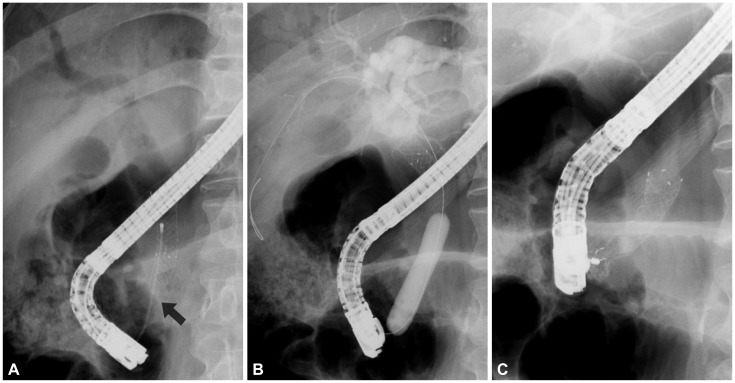
A 62-year-old man with benign biliary stricture due to chronic pancreatitis underwent 10-mm diameter, 60-mm lengthened covered biliary SEMS (Shim-Hanaro; MI Tech, Seoul, Korea) (Fig. 1). After 5 months, removal of SEMS was attempted by using forcep to grasp the extraductal portion of the distal SEMS. During the procedure, duodenal end of the stent broke (Fig. 2), and remnant SEMS moved proximally into the common bile duct (Fig. 3A). Despite multiple trials were attempted to retrieve the remnant SEMS by using various grasping accessories or balloon catheter, methods failed. Endoscopic papillary balloon dilatation with maximal diameter of 12 mm diameter (CRE wire-guided dilator; Boston Scientific, Marlboro, MA, USA) was performed below the remnant SEMS to make a space between the outer surface of SEMS and the inner surface of common bile duct (Fig. 3B). Snare was advanced through the space, then the stent was grasped and retrieved without any complication (Fig. 3C). The Fig. 4 shows the whole feature of removed stent with fracture.
DISCUSSION
The frequency of SEMS using is gradually increasing in alternative treatment for benign biliary strictures.3 It is difficult to remove uncovered SEMS coated with epithelial hyperplasia. In comparison, it is easier to remove covered SEMS.1,4 Therefore, recently, the frequency of covered SEMS using is increasing. Complications related to SEMS are failure of stent release, malpositioning of the stent, stent occlusion with epithelial hyperplasia, duodenal bleeding or perforation due to trauma to duodenal wall, stent fracture and stent migration. The causes of fracture were not only therapeutic thermal overstrain during the electrocoagulation but spontaneity.2,5,6 The fracture might be related to bile induced corrosion or metal fatigue from constant and repeated bending in the duodenum.5-7 The anatomic sites of fracture were mostly around the ampulla,5-7 and a literature7 reported that 75% (3/4) of the fracture sites were at the ampulla with disconnection of the distal part of the stent in patients with periampullary malignant biliary obstruction. The cause of fracture of SEMS in this case was unclear and might be multifactorial. In case of distal biliary stricture, it could be suggested that there is a possibility of the structural characteristics of weak point of the SEMS at the ampulla as a causative factor. To the best of our knowledge, fracture of SEMS during the endoscopic removal has of been previously reported. In our case, the fracture of distal part of stent at the level of ampulla occurred during the retrieval of the normally situated SEMS. We presume that the event related to shearing force by pulling the stent through the grasp device at the damageable site of unseen stress fracture.
All types of biliary stents could have a risk for the complication of migration. Biliary stent migration can reduce the function of stent and make injury of duodenal wall, perforation, or bleeding.8 If stent migration occurred, the stent should be removed. In the case of retrieval of distally migrated SEMS, snare or forcep can be used to grasp the free end of SEMS.3 However, it is difficult to remove proximally migrated biliary SEMS, and methods to remove proximally migrated SEMS are stent cannulation and subsequent balloon retrieval, balloon placement parallel to the stent with traction retrieval, and use of a wire basket, snare, or forceps.9-11 In our case, we successfully removed the distal fragment of the fractured SEMS at the beginning, but we failed to remove proximally migrated fragment of the fractured SEMS with use by several tools such as the forcep, snare, balloon, or retriever. Therefore, to grasp firmly remained stent, we allocated spaces between the SEMS and inner part of bile duct through the balloon, then successfully we removed the stent. In our case, we realized that the endoscopist must be careful to inspect the complication such as the fracture and migration of stent which can occur during the endoscopic removal of SEMS.