INTRODUCTION
A squamous papilloma is occasionally found in the esophagus by endoscopic examination. However, a squamous papilloma of the stomach is very rare. A squamous papilloma is a benign proliferation of the stratified squamous epithelium that is found in the skin, mouth, throat, esophagus, genitalia, or anal canal. The pathogenesis of esophageal squamous papilloma remains unclear, although roles for human papilloma virus (HPV) infection and chronic mucosal irritation have been proposed.
So far, only three cases of gastric papilloma have been reported,1,2,3 and in all these cases, the cause of gastric squamous papilloma has not been determined. In this case, the papilloma was located at the cardia, which is a region where an island of squamous epithelium is known to occur.4 Another factor could be squamous metaplasia. Squamous metaplasia of the stomach can occur during the healing of inflammatory conditions.5 Although it is unknown whether repeated detriments to the island of squamous epithelium or gastric squamous metaplasia lead to papillomas like esophageal squamous papillomas, we presumed that it may account for some instances of gastric squamous papilloma.
Until now, to the best of our knowledge, endoscopic resection of a squamous papilloma of the stomach has not been reported, although there are a few case reports concerning squamous papilloma in this organ. Herein, we report a case of gastric squamous papilloma, which was successfully removed by endoscopic resection.
CASE REPORT
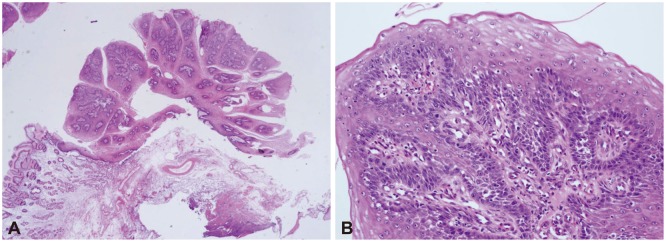
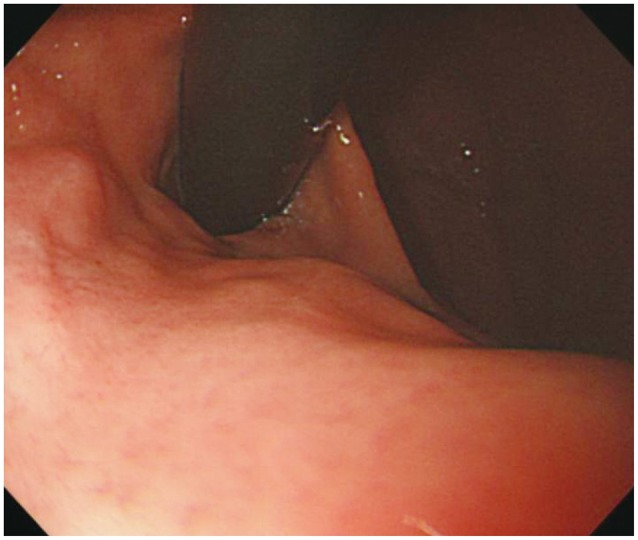
An asymptomatic 52-year-old woman was referred to Pusan National University Yangsan Hospital for evaluation of a polyp detected by endoscopy. She had neither a history of operations nor a medical history of conditions such as diabetes, hypertension, hepatitis, or tuberculosis. She drank alcohol in moderation and did not smoke. An initial endoscopic evaluation for a routine health check up at the local hospital revealed a 1-cm sized Is polyp with hyperemic change in the cardia. A second endoscopy was performed in our institution and showed a 1-cm sized polyp originating from the cardia just below the esophagogastric junction, with a whitish granular surface in the front view (Fig. 1A) and a hyperemic surface in the retroflex view (Fig. 1B). Biopsy samples taken from the lesion revealed squamous epithelium-lined, inflamed mucosa showing papillary growth, which is suggestive of squamous papilloma. She subsequently underwent an endoscopic mucosal resection and no procedure-related complications occurred. The specimen had a characteristic verrucous appearance (Fig. 2). Histological analysis of the resected specimen showed proliferation of the squamous epithelium without atypia, accompanied by a papillary projection with a fibrovascular core, which is consistent with papilloma. Surrounding tissues containing foveolar epithelium revealed that the polyp originated in the stomach, thus confirming the diagnosis of gastric squamous papilloma (Fig. 3). HPV DNA was Papillomanot detected in the resection specimen. Six months later, endoscopy showed complete healing of the mucosa without residual papilloma or recurrence (Fig. 4).
DISCUSSION
Gastric polyps are locally elevated lesions protruding into the gastric lumen and incidentally discovered in about 2% of endoscopic examinations.6 These polyps are usually salmon pink or red in appearance during endoscopy and they are sessile, semipedunculated, or pedunculated in shape. The most common gastric polyps are fundic gland polyps, while hyperplastic polyps are the second most common gastric polyps, and include sentinel hyperplastic polyps on esophagogastric junctions.7 Gastric adenoma and inflammatory fibroid polyps can also be considered gastric polyps. Only a few cases of squamous papillomas of the stomach have been reported. The endoscopic finding of the papilloma in this case was elevated mucosa with a whitish granular surface in the front view and a hyperemic surface in the U-turn view, as compared with the adjacent mucosa. It is difficult to distinguish between a papilloma on the cardia and a sentinel polyp depending only on endoscopic findings, but small erosions, ulcerations, or plaques are commonly seen on the surface of sentinel polyps. Application of Lugol's iodine solution also helps to identify squamous papilloma, because it stains the papilloma brown like normal esophageal mucosa.
Squamous papilloma is a benign proliferation of the stratified squamous epithelium that is found in the skin, mouth, throat, esophagus, genitalia, or anal canal. Most squamous cell papillomas in the gastrointestinal tract are identified in the distal esophagus, as solitary lesions, although patients with over 10 lesions have also been reported.8 Esophageal squamous papilloma usually presents as a small, single, whitish-pink, round, sessile mass with numerous finger-like projections at the surface, and histologically, it is characterized by benign proliferation of stratified squamous epithelium, resulting in a papillary or verrucous exophytic mass.9 In contrast with esophageal squamous papilloma, the endoscopic finding in this case was a polypoid lesion with hyperemic change in the retroflex view. The stomach is a very rare site for squamous papilloma, because a squamous papilloma does not normally arise in the normal gastric columnar epithelium. In this case, arguments regarding whether the papilloma originates from the stomach can be made, but the lesion was clearly located at the cardia just below the esophagogastric junction according to endoscopy, and the tissues surrounding the papilloma had foveolar epithelium, which is suggestive of a stomach origin.
The origin of squamous papilloma in the stomach can be analogized to squamous cell carcinoma of the stomach. The pathogenesis of squamous cell carcinoma of the stomach is not clear, but five main theories have been proposed including: (1) nests of ectopic squamous cells in the gastric mucosa; (2) squamous metaplasia of the gastric mucosa before malignant transformation; (3) squamous differentiation in a preexisting adenocarcinoma; (4) multipotential stem cells in the gastric mucosa; and (5) gastric vascular endothelial cells.10 Squamous metaplasia has been described in healing gastric ulcers and a variety of conditions associated with long-standing chronic inflammation.11 An island of squamous epithelium has been known to occur near the cardia.4 The pathogenesis of gastric squamous papilloma is deduced from esophageal squamous papilloma. The etiology is uncertain, but roles for chronic mucosal irritation and HPV have been proposed.12,13 Taking all the circumstances into consideration, we presumed that squamous papilloma in the stomach arises from squamous metaplasia or the island of squamous epithelium and is triggered by chronic inflammation resulting from environmental stimuli.
Whether a squamous papilloma in the gastrointestinal tract should be treated is controversial. A squamous papilloma of the distal esophagus does not change into a malignant neoplasm, although a squamous papilloma of the larynx or the cervix may be associated with squamous cell carcinoma.14,15 Esophageal squamous papillomas are benign epithelial lesions and do not cause symptoms, although large lesions can cause dysplasia.16 Oropharyngeal squamous papillomas are also considered benign epithelial lesions; however, there is one case report of malignant change in this context.17 We did not know whether the origin of squamous epithelium in this case was squamous metaplasia, but gastric squamous metaplasia does have the potential to become gastric squamous cell carcinoma.10
As gastric squamous papilloma is clinically extremely rare, no information is available about its history or optimal treatment. Endoscopic resection of a gastric papilloma is not difficult. Therefore, we recommend endoscopic resection for patients with gastric squamous papilloma. If endoscopic resection is not feasible, endoscopic surveillance should be considered, even though it is likely to have a benign course. In this case, the lesion was completely removed by endoscopic resection, and there was no evidence of recurrence in follow-up endoscopy after 6 months.
In summary, if a gastric polyp is observed, especially in the cardia, squamous papilloma should be considered in the differential diagnosis. The prognostic value of squamous papilloma has not been explained because its incidence is rare. Therefore, we recommend endoscopic resection for treatment of squamous papilloma in the stomach when possible.