INTRODUCTION
Cavernous hemangiomas in the gastrointestinal (GI) tract are rare in children.1234 These tumors are usually asymptomatic for a long time, often being diagnosed as an incidental finding or during investigative procedures for other disorders.34567 Cavernous hemangiomas are mainly found in the upper and lower GI tract, and they rarely occur in the small intestine.12348 The most common clinical presentation is GI bleeding;2 the major symptom of hemangioma of the small intestine is occult or overt GI bleeding.5
The diagnosis of cavernous hemangiomas are usually made by using computed tomography (CT), magnetic resonance imaging (MRI), barium swallow study, double-balloon enteroscopy, or capsule endoscopy in patients with obscure or overt bleeding.2 The diagnosis is extremely difficult because small bowel hemangiomas are rarely demonstrable. Radiological methods show low accuracy in detecting the origin of a hemangioma in the small bowel.1 In recent years, capsule endoscopy has been used to diagnose small bowel lesions in patients with obscure and overt GI bleeding.3910
In the domestic literature, there is only one report of a small bowel hemangioma in a child;11 in this previous report of a 2-year-old boy with severe iron-deficiency anemia and gross GI bleeding, a small bowel hemangioma was detected during an exploratory laparotomy. Herein, this is the first domestic report of a case of cavernous hemangioma of the small intestine diagnosed with capsule endoscopy with no evidence of gross GI bleeding.
CASE REPORT
A 13-year-old boy came to the hospital with symptoms of nausea and dizziness for a week. The patient had no symptoms of hematemesis or bloody stool. At the time of physical examination in the hospital, the patient was conscious and his conjunctiva was pale. The abdomen showed no distension, flank pain, masses, or organomegaly. There were no bleeding tendencies such as purpura, petechial rash, or skin bruising. The physical examination revealed no other specific signs.
An analysis of the patient's previous history revealed that recurrent episodes of severe iron-deficiency anemia had been treated with blood transfusion and iron supplements since the age of three years. These symptoms had improved transiently upon treatment. However, he had defaulted on subsequent follow-up.
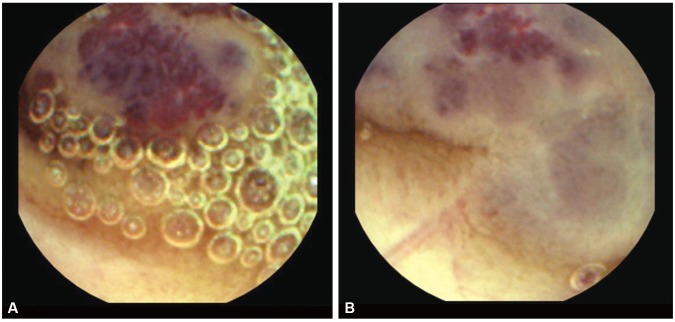
A complete blood count showed an hemoglobin (Hb) level of 6.6 g/dL, mean corpuscular volume of 73.9 fL, mean corpuscular hemoglobin of 21.5 pg, hematocrit of 22.7%, white blood cell count of 5,400/mm3 with 87.9% neutrophils, and platelet count of 444,000/mm3. Urinalysis and a stool examination did not indicate blood loss. The analyses for iron-deficiency anemia showed ferritin levels of 3.1 ng/mL, serum iron levels of 191 ┬Ąg/dL, total iron-binding capacity of 342 ┬Ąg/dL, and transferrin levels of 295 mg/dL. Results of gastroduodenoscopy, colonoscopy, and Meckel scans were negative. To obtain a definite diagnosis and find the obscure bleeding focus, the patient underwent capsule endoscopy. Capsule endoscopy showed a purple-colored polypoid mass with surface bleeding in the jejunum (Fig. 1).
At that point, obscure bleeding resulting in refractory iron-deficiency anemia could not be ruled out. Excision of the mass, about 140 cm below the Treitz ligament, was performed successfully (Fig. 2). Macroscopically, the surgical specimen was a 4.2├Ś5.2-cm hemangioma involving the entire layer of the intestinal wall, and it consisted of spongy-like spaces filled with blood clots (Fig. 3). Microscopically, the tumor consisted of irregular dilated, blood-filled vessels lined by flattened endothelium (Fig. 4). Histology indicated that the tumor was a cavernous hemangioma.
The patient was discharged 7 days postsurgery. During the 3 years of follow-up postsurgery, the patient was healthy and did not experience anemia. The patient's Hb level was 14.6 g/dL.
DISCUSSION
Hemangiomas in the small intestine are very rare benign tumors that account for approximately 5% of all GI neoplasms.12 Typically, they occur in the ileum.4 The lesions are rarely found in children; only a few cases have been reported in the literature. The major symptom of hemangioma of the small intestine is overt GI bleeding.2 Less commonly, cavernous hemangioma in the small bowel may present with different chronic or obscure types of GI bleeding.4 Occasionally, an obstruction may be the initial finding.
Preoperative diagnosis is extremely difficult because small hemangiomas are rarely demonstrable. Traditional techniques to investigate the small intestine include CT, MRI, barium swallow study, double-balloon enteroscopy, or capsule endoscopy.212 However, these often lack accuracy.11213 In the current case, the patient had recurrent and severe anemia without evidence of gross GI bleeding, and the purplish stalked mass in the small bowel was diagnosed with capsule endoscopy. The mass was a solitary cavernous hemangioma, which is seldom identified with the usual methods such as CT or upper and lower GI endoscopy.
Internationally, there have been about five cases of solitary cavernous hemangioma of the small bowel along with long-standing iron-deficiency anemia and no gross GI bleeding.126814 Three of the five cases developed in children,1814 and two of these three cases showed the same clinical manifestation and were diagnosed with capsule endoscopy as in this case.114 One of these three cases showed the same clinical features as this case, but it was diagnosed with Technetium-99m red blood cell scintigraphy.8 Only two cases of cavernous hemangioma of the small bowel have been reported domestically. Kye et al.15 reported of an 81-year-old female patient who presented with nausea, dizziness, and intermittent melena for three months; in this case, a mass in the small bowel was diagnosed with CT. She had undergone an explorative laparotomy, and histology revealed a cavernous hemangioma. Park11 performed explorative laparotomy on a 2-year-old boy with melena and severe iron-deficiency anemia since 18 months. He had been symptomatic with gross GI bleeding. The patient was likewise diagnosed with a small bowel cavernous hemangioma. The previously reported patients1115 developed overt GI bleeding and they were treated by utilizing different diagnostic techniques than the presented case.
Small bowel lesions can be detected at similar success rates with capsule endoscopy and double-balloon endoscopy.9 Double-balloon enteroscopy is a sensitive diagnostic tool.16 Although the procedure is a useful method for diagnosis, it is more suited for adult patients with small bowel abnormalities than for children, as the outer diameter of the double-balloon enteroscope is 12.2 mm, which could be very uncomfortable for children. Complications of the method, including postprocedural abdominal pain, GI tract tears, and acute pancreatitis, have been reported in children.16 However, capsule endoscopy helps to identify the leading causes of obscure GI bleeding in all age groups.9171819
Capsule endoscopy is superior to push enteroscopy and small bowel barium radiography for the diagnosis of clinically significant small bowel pathologies in patients with obscure GI bleeding.7 When patients have recurrent and severe anemia with no evidence of gross bleeding, obscure GI bleeding of the small bowel should be considered in the differential diagnosis.91720
In conclusion, capsule endoscopy may be a reasonable alternative diagnostic tool for small hemangiomas with chronic GI blood loss among children, especially in those with accompanying diseases that are difficult to differentiate, as reported in the present case.