Practice Patterns and Use of Endoscopic Retrograde Cholangiopancreatography in the Management of Recurrent Acute Pancreatitis
Article information

Abstract
Background/Aims
There are conflicting opinions regarding the management of recurrent acute pancreatitis (RAP). While some physicians recommend endoscopic retrograde cholangiopancreatography (ERCP) in this setting, others consider it to be contraindicated in patients with RAP. The aim of this study was to assess the practice patterns and clinical features influencing the management of RAP in the US.
Methods
An anonymous 35-question survey instrument was developed and refined through multiple iterations, and its use was approved by our Institutional Review Board. The survey was distributed via email to 408 gastroenterologists to assess the practice patterns in the management of RAP in multiple clinical scenarios.
Results
The survey was completed by 65 participants representing 36 of the top academic/tertiary care centers across the country. Approximately 90.8% of the participants indicated that they might offer or recommend ERCP in the management of RAP. Multinomial logistic regression analysis revealed that ductal dilatation and presence of symptoms were the most predictive variables (p<0.001) for offering ERCP.
Conclusions
A preponderance of the respondents would consider ERCP among patients with RAP presenting to tertiary care centers in the US. Ductal dilatation, presence of symptoms, and pancreas divisum significantly increased the likelihood of a recommendation for ERCP.
INTRODUCTION
Recurrent acute pancreatitis (RAP) is generally defined as the presence of two or more episodes of AP without concomitant clinical and/or radiographic evidence of chronic pancreatitis [1]. The estimated incidence of AP is between 15 and 45 per 100,000 persons per year, with a risk of recurrence of nearly 20% [1-6]. While gallstone diseases and alcohol exposure are generally accepted as the two primary causes of RAP, other etiologies, including autoimmune, hereditary, metabolic, and anatomic variants and Sphincter of Oddi dysfunction (SOD), are also considered [7]. It has been estimated that up to 30% of episodes of RAP are idiopathic in nature [8].
The management of RAP has become a topic of debate, particularly among gastroenterologists, interventional endoscopists, and medical pancreatologists. Some gastroenterologists recommend endoscopic retrograde cholangiopancreatography (ERCP) in this setting, while some do not [9]. Among patients who undergo ERCP, the specific procedural intervention may vary widely, including biliary sphincterotomy, pancreatic sphincterotomy, pancreatic stent placement, manometry, and minor papilla therapy for divisum depending on the clinical context, local practice, and physicians’ preference [10-18]. These more invasive strategies may follow an extensive diagnostic evaluation with laboratory testing, imaging with computed tomography and/or magnetic resonance imaging or cholangiopancreatography with or without secretin enhancement, endoscopic ultrasound (EUS), and Sphincter of Oddi manometry [13].
In the setting of RAP, it is unclear which patients are being referred for ERCP. In patients who undergo ERCP, it is unclear which interventions are being performed. To consider the proper approach to RAP and to develop the proper trials to determine the appropriate management, it is critical to understand the current practice patterns. Within a subgroup of patients referred for ERCP, it is important to clarify the specific procedural approaches that are being employed. This study examined the national practice patterns for patients presenting with RAP.
MATERIALS AND METHODS
Overview
The study protocol was reviewed and was approved by the Institutional Review Board (IRB) at the Emory University School of Medicine.
Survey instrument
A 35-question survey instrument was developed and refined through multiple iterations to assess the current practice of gastroenterologists in the management of RAP. The final survey was approved by the IRB. The first nine questions assessed demographics, respondent training, type of practice, and experience with ERCP. A total of 20 questions asked the respondents to consider ERCP in the management of RAP considering various factors, including presence of symptoms, pancreatic ductal dilatation, and history of pancreas divisum. Additional questions assessed how alcohol drinking and smoking history may influence the management (Appendix).
Participants
The survey instrument was distributed via email to 408 gastroenterologists who were identified as leaders in their respective fields in various programs across the US. Emails were sent out two additional times, i.e., at 3 and 6 weeks, to maximize the response rates. An online consent/information sheet, as confirmed by the IRB at the Emory University School of Medicine, accompanied each email that was sent. Consent to participate in the study was determined from voluntary completion of the survey. No additional personal identifiers or any independent information regarding the participants were collected. Responses were collected using a survey tool from Google Forms (Alphabet Inc., Mountain View, CA, USA).
Statistical analysis
The standard χ2 test and Fisher’s exact test were used for comparisons between groups. Multinomial logistic regression testing was conducted to analyze further the effects of multiple variables, including ductal dilatation, pancreas divisum, symptomatology, and sex, on the decision to offer or recommend ERCP. All p-tests were two-sided, and a p-value of <0.05 was considered statistically significant. Statistical analysis was performed using the statistical software JMP Pro 13 (SAS, Cary, NC, USA).
RESULTS
Respondent demographics
The survey was completed by 65 participants (15.9%) representing 36 different academic/tertiary centers across the country, with 87.7% identified as having been in practice for at least 6 years and 52.3% performing at least 250 ERCPs each year. Additionally, 73.8% of the respondents were identified as a pancreatologist or specialized in pancreatology, and 70.8% had completed a fellowship training in advanced endoscopy. Their demographics are summarized in Table 1.
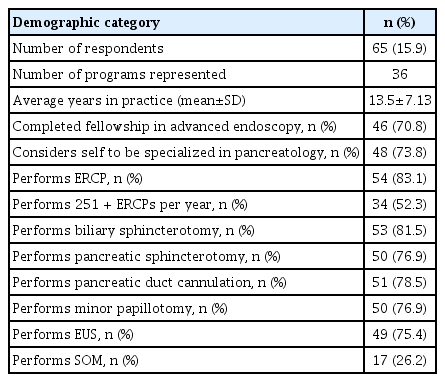
Demographic Features of Survey Respondents
Practice patterns
The respondents were asked to indicate their estimate of the most common etiologies for RAP. In response, 38.5% of the participants reported that alcohol abuse was the primary etiology of RAP in their cohort, while 35.4% reported an idiopathic etiology. Similarly, 38.5% of the respondents noted that greater than or equal to two episodes of RAP were needed before intervening with ERCP, with another 20% believing that greater than or equal to three episodes of RAP were required; further, 33.8% claimed that the number of episodes of RAP did not influence their decision to offer or recommend ERCP.
Approximately 90.8% of the participants reported that they might offer or recommend ERCP in the management of RAP. For patients with pancreatic ductal dilatation and pancreas divisum, 95.4% (p<0.001) might offer ERCP (Table 2).

Univariate Analysis of Dilatation and Pancreas Divisum on Endoscopic Retrograde Cholangiopancreatography
Multinomial logistic regression testing was performed to characterize further the impact of ductal dilatation, pancreas divisum, pancreatic-type symptomatology (e.g., epigastric pain), and sex on the decision to offer or recommend ERCP (Table 3, Fig. 1). The respondents were most likely to recommend ERCP in symptomatic female patients with pancreas divisum and pancreatic ductal dilatation (96.9%, p<0.001), with 92.3% (p<0.001) indicating that they would offer ERCP to male patients in the same scenario. For asymptomatic female patients with pancreas divisum and pancreatic ductal dilatation, 72.3% (p=0.005) of the respondents would offer ERCP; conversely, 78.5% (p<0.001) would offer ERCP to male patients in the same scenario. Taken together, pancreatic ductal dilatation and presence of pancreatic-related symptoms were the most predictive variables for a recommendation for ERCP (p<0.001; Fig. 2). Pancreas divisum was significantly associated with the decision to offer or recommend ERCP (p=0.012), while sex was not (p=0.34).
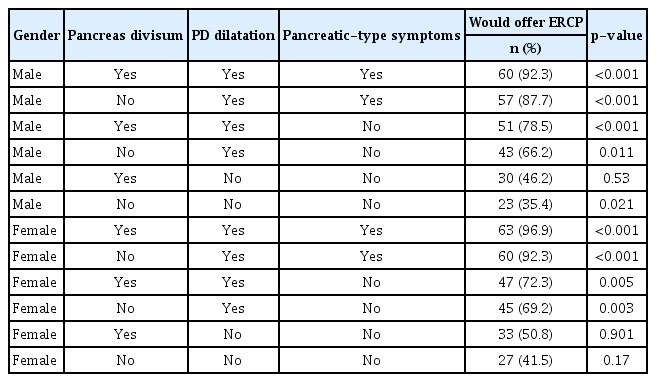
Multinomial Logistic Regression on the Recommendation to Offer Endoscopic Retrograde Cholangiopancreatography
Proportion of respondents who would offer endoscopic retrograde cholangiopancreatography (ERCP) considering different factors. The more factors a patient had—including the presence of pancreatic ductal dilatation (e.g., 6 mm), a history of pancreas divisum, and the presence of pancreatic-type pain—the higher the response rate for ERCP.

Graphical representation of the multinomial logistic regression testing assessing the impact of several clinical features on the recommendation to offer endoscopic retrograde cholangiopancreatography (ERCP) in patients with recurrent acute pancreatitis. Pancreatic ductal dilatation appeared to be the single most impactful factor, followed by symptomatology. PD, pancreatic duct.
There was heterogeneity in the specific interventions during ERCP. At the initial intervention of patients without pancreatic ductal dilatation, 45.9% would offer biliary sphincterotomy; 11.5%, pancreatic sphincterotomy; and 32.8%, both. In patients with pancreatic ductal dilatation, 66.2% might perform pancreatic sphincterotomy; 52.3%, biliary sphincterotomy; and 32.8%, both; further, 95.4% noted that they would also offer EUS in this scenario (Table 4).

Specific Interventions in the Management of Recurrent Acute Pancreatitis with a Dilatated Pancreatic Duct Compared to Non-Dilatated Pancreatic Duct
DISCUSSION
The proper management of RAP remains controversial. Some providers recommend ERCP, while some suggest that ERCP should be avoided in patients with pancreatitis. Within groups of patients referred for ERCP, there is also considerable heterogeneity in the specific approaches taken. This study investigated the practice patterns and the use of ERCP in the management of RAP in a large sample of practitioners treating patients with pancreatic diseases in the US. We found that a high proportion of gastroenterologists (90.8%) would consider ERCP for patients presenting with RAP. Several factors increased the likelihood of a recommendation for endoscopic intervention, including ductal dilatation, divisum, and presence of symptoms. Some factors, such as sex, were not significant. In patients undergoing ERCP, a small proportion (45.9%) would perform biliary sphincterotomy as the first intervention; however, the specific approaches taken at the index ERCP varied. In the US, gastroenterologists are likely to consider ERCP as a therapeutic modality for patients presenting with RAP.
A number of factors may influence a practitioner’s decision to recommend ERCP, including the presence of pancreatic ductal dilatation (e.g., 6 mm), history of pancreas divisum, and presence of pancreatic-type pain. The more factors that a patient had, the higher the response rate for ERCP (Fig. 1). For example, 95.4% of the respondents would consider recommending ERCP when a patient had either pancreatic ductal dilatation or a history of pancreas divisum. While 96.9% of the respondents would offer or recommend ERCP to a patient with pancreatic ductal dilatation, a history of pancreas divisum, and abdominal symptoms, only 35.4% would consider ERCP in a patient with a normal duct, no history of pancreas divisum, and no symptoms. Among all the factors studied, pancreatic ductal dilatation appeared to be the single most impactful factor, followed by symptomatology. While pancreas divisum was significantly associated with a recommendation for ERCP, it was a weaker predictor (Table 3, Fig. 2).
Sex was not a significant factor in the decision to offer ERCP. Generally, the respondents were somewhat more likely to recommend ERCP in female patients relative to male patients with a similar presentation. For example, 96.9% of the respondents would offer ERCP to a female patient with ductal dilatation, symptomatology, and a history of pancreas divisum compared with 92.3% recommending such to a male patient in the same scenario. Some studies have identified female sex to be a significant risk factor for post-ERCP pancreatitis, while others have not [19-27]. However, there are no available data on the differential outcomes following ERCP according to sex.
The respondents also indicated the specific approaches they would take during ERCP (Table 4). At the initial intervention of patients without pancreatic ductal dilatation, 45.9% of the respondents would offer biliary sphincterotomy. A retrospective study found that biliary sphincterotomy alone may be as effective as other interventions [16]. Among patients with pancreatic ductal dilatation, 66.2% might perform pancreatic sphincterotomy; 52.3%, biliary sphincterotomy; and 32.8%, both; moreover, 95.4% noted that they would also offer EUS in this scenario (Table 4). Previous studies have suggested that a dilated duct may be associated with greater clinical success in ductal cannulation compared with a normal-sized duct [28,29], and ductal dilatation is often considered to indicate an obstructive process, which might be mitigated by ERCP.
Among patients with both RAP and a history of pancreas divisum, some approaches—including minor papilla stenting—have yielded success rates of 91.7% in limiting or improving symptoms, including reduced rates of pancreatic-type pain, hospitalization, or pancreatitis [11,12,30]. Other studies addressing ERCP in patients with idiopathic RAP or SOD reported an efficacy rate of 42%–89% when analyzing the role of biliary stenting, pancreatic stenting, or both [16,31-35]. In patients with SOD, studies have reported similar efficacy with biliary stenting and dual stenting [16]. While many respondents would recommend ERCP in some settings for patients with RAP, there is considerable heterogeneity in the specific approach, which would be taken at the index ERCP. An ongoing prospective clinical trial may provide relevant information on the outcomes of interventions for patients with divisum [36]; similar work may be indicated for RAP with conventional ductal anatomy.
There were a number of limitations in this study. Selection and recall biases are possible given the subjective nature of the survey approach. While this anonymous IRB-approved survey instrument was sent to a large number of gastroenterologists across the country, the majority who responded (70.8%) had completed a fellowship training in advanced endoscopy. Nearly three-quarters were identified as a pancreatologist or specialized in pancreatology, and over half performed over 250 ERCPs each year in their practice. Thus, there may be limitations in the generalizability of the findings to the larger community outside of the tertiary care setting. Inherent in a practice survey design, there may be differences in the perception of practice approaches and actual providers’ practice. There has been no available validated survey instrument that could capture specific data on the decision to offer ERCP in RAP and that could evaluate the specific procedural interventions performed in patients undergoing such. Therefore, as with other surveys in endoscopic practice [17], an original survey instrument was developed.
In conclusion, this study found that ERCP is often recommended in tertiary care institutions for patients presenting with RAP. Some factors, such as ductal dilatation and presence of symptoms, significantly increased the likelihood of ERCP recommendation. There was considerable heterogeneity among the specific interventions performed at the index ERCP. These data highlight the need to determine the subset of patients for whom ERCP may be beneficial and what approaches are the most effective. While the consensus definitions are clear, our understanding of the management for patients with RAP is evolving.
Notes
Conflicts of Interest: The authors have no financial conflicts of interest.
Acknowledgements
The authors would like to thank the following physicians and staff for their invaluable input and assistance in this project. Venkata Akshintala, Harry Aslanian, Augustin Attwell, Todd Baron, Alin Botoman, James Buxbaum, Lisa Cassani, Amitahb Chak, Jennifer Christie, Victor Ciofoaia, Gregory Cote, Peter Cotton, Sarah Cristofaro, Christopher DiMaio, David Desliets, Peter Draganov, Steven A. Edmundowicz, Grace Elta, Jeffrey Easler, Joseph Elmunzer, Evan Fogel, David Forcione, Christopher Forsmark, A. Jay Freeman, Martin Freeman, Anthony Gamboa, Timothy Gardner, Gregory Ginsberg, Wendy Ho, Brian Jacobson, Kunal Jajoo, Michel Kahaleh, Peter Kelsey, Jason Klapman, Michael Kochman, Christopher Lind, Robert Lockwood, Raimondo Massimo, Klaus Mönkemüller, Daniel Mullady, Jose Nieto, Keith Obstein, Mohamed Othman, Georgios Papachristou, Octavia Pickett-Blakely, Teodor Pitea, Douglas Pleskow, John Poneros, Gottumukkala S. Raju, John Saltzman, James Scheiman, Amrita Sethi, Janak Shah, Raj Shah, Ali Siddiqui, Vikesh Singh, Mahir Waghi, Michael Wallace, Andrew Wang, Sachin Wani, Rabindra Watson, C. Mel Wilcox and Patrick Yachimski.