INTRODUCTION
Angiolipoma is a benign neoplasm composed of adipose tissue and proliferative vascular components. These lesions commonly present as encapsulated subcutaneous tumors of the limbs and trunk [1]. Angiolipoma in the gastrointestinal tract is extremely rare [2], and the final diagnosis generally depends on histological examination of the excised specimen.
Most previous cases that have been reported were diagnosed and treated with surgical management [3-6], and only one case was treated with endoscopic mucosal resection (Table 1) [3]. Herein, we reported a case that was diagnosed as an extensive gastric angiolipoma and was treated with endoscopic submucosal dissection (ESD).
CASE REPORT
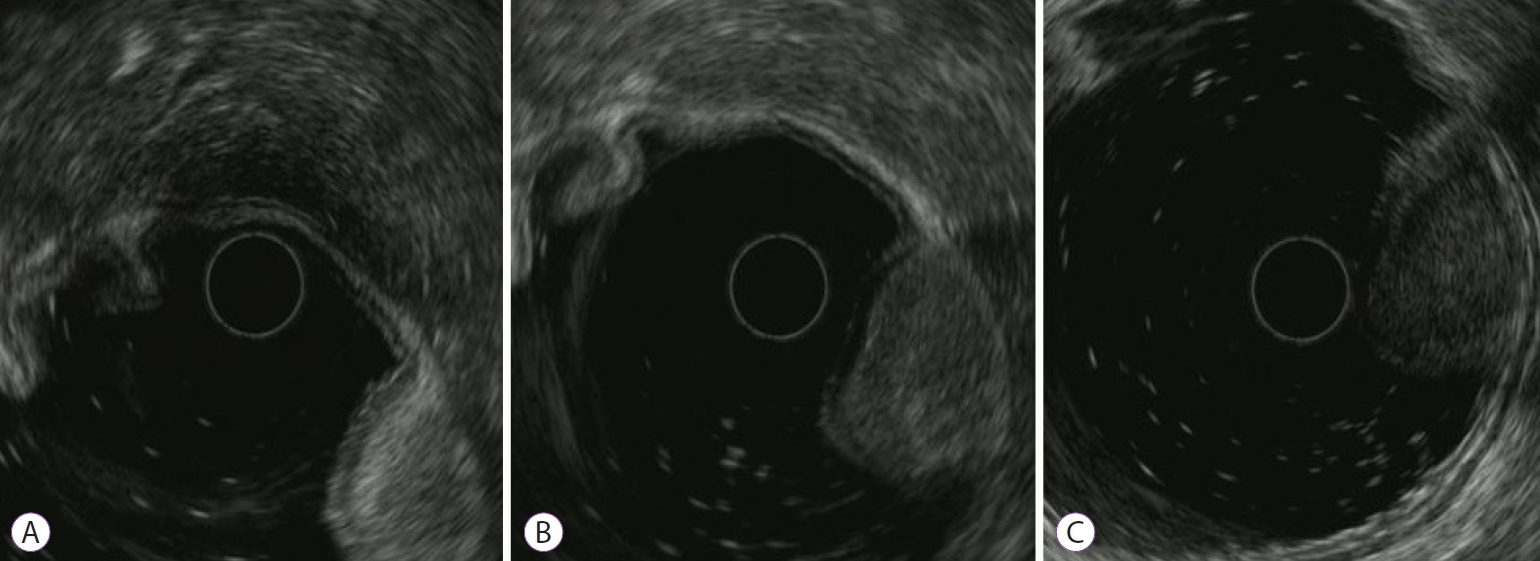
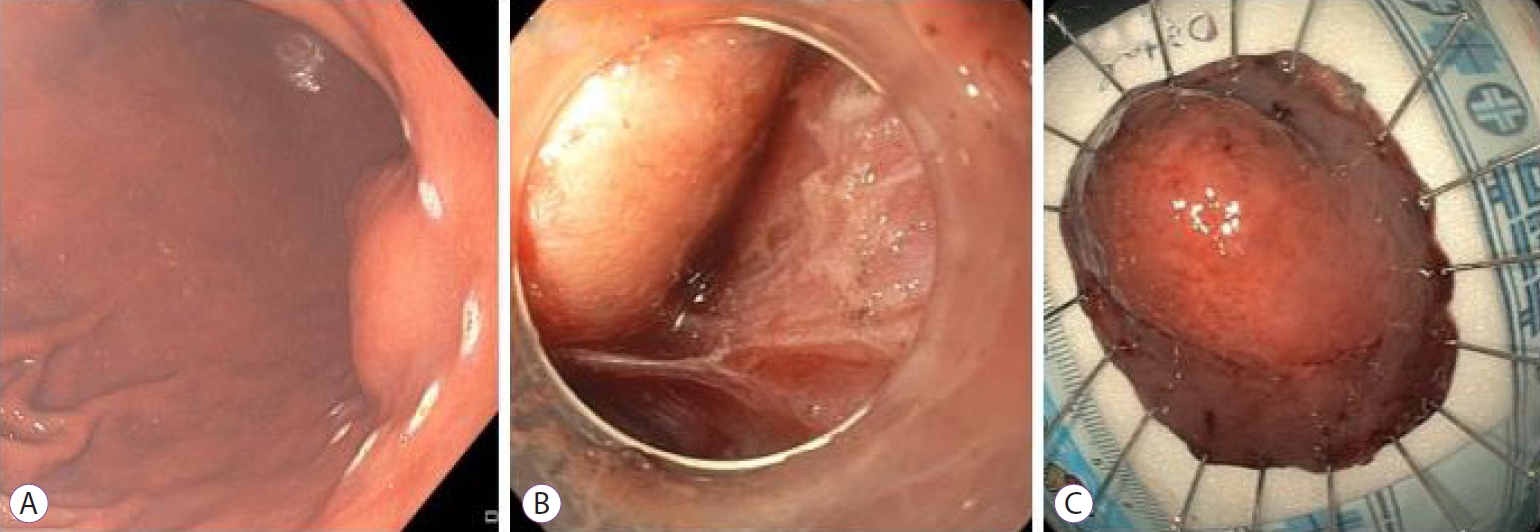
A healthy 46-year-old man underwent esophagogastroduodenoscopy (EGD) during a general examination. A subepithelial lesion, approximately 4 cm, with a cushion sign covered with mucosa and a patchy area of redness was seen at the lesser curvature of the lower body of the stomach (Fig. 1). An endoscopic biopsy was obtained from the red colored area of the mucosa of the lesion. The biopsy specimen was limited to the superficial mucosa and revealed only chronic inflammation. Although abdominal computed tomography (CT) showed fat tissue density, endoscopic ultrasound (EUS) showed a heterogeneous oval lesion, approximately 4 cm in size, that originated from the third layer (Fig. 2). Depending on the location of the EUS, the echogenicity of the lesion had changed from hyperechoic (Fig. 2A) to isoechoic (Fig. 2B) and to hypoechoic (Fig. 2C). Thus, it was assumed that the lesion might be an unusual type of lipoma, and we planned to resect the lesion with ESD for accurate diagnosis and treatment.
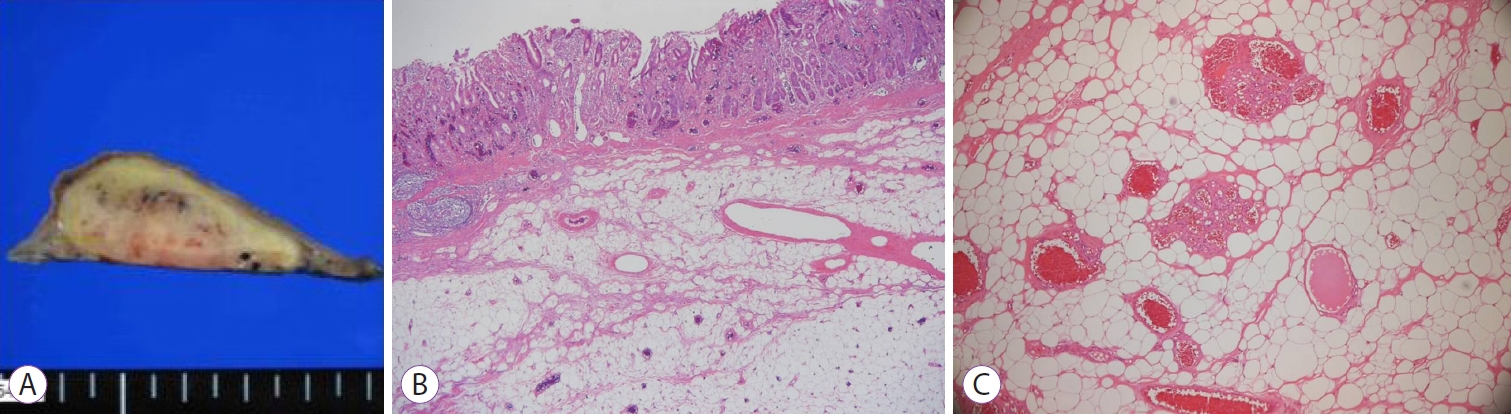
The patient was admitted, and the laboratory tests showed a normal hemoglobin level of 15.5 g/dL and hematocrit of 45.5% with other biochemical tests within normal ranges. The gastric subepithelial tumor (SET) was resected using ESD (Fig. 3). The entire tumor was successfully removed, and the resection margin was clear. The specimen was a SET measuring 3.9У1.6 cm (Fig. 4A). Histological tests showed a tumor in the submucosa consisting of mature adipose tissue interspersed with capillaries (Fig. 4B). The lesion showed prominent vascular components composed of several dilated capillaries (Fig. 4C). Based on the histological findings, the patient was diagnosed with gastric angiolipoma.
The patient had no specific complications from ESD and was discharged 2 days after the procedure.
DISCUSSION
Angiolipoma was first defined in 1912 and was first described as a new disease entity in 1960 due to its different clinical and pathological features from those of lipoma [7]. Angiolipomas are generally subcutaneous and encapsulated and most commonly occur on the trunk and extremities [1,5]; they are rarely found in the stomach [8-10]. In a literature review, only five cases of angiolipoma involving the stomach have been reported [3,8-11]. Four cases of gastric angiolipomas presented with anemia and bleeding, and one case showed no significant findings on EGD during the general examination.
Gastrointestinal angiolipomas can be detected by endoscopy or imaging methods, such as EUS or CT, before histopathological diagnosis [12,13]. In the endoscopic examination, gastrointestinal angiolipomas are usually seen as focal mucosal thickening. Yellowish-pink mucosa with or without superficial erosions may be seen, but these are non-specific findings. A lipoma is typically identified during EUS as a hyperechoic lesion observed in the submucosal layer. However, in gastrointestinal angiolipomas, EUS may show as either hyperechoic or isoechoic lesions in the submucosal layer [9,13,14]. In our case, the EUS finding changed from hyperechoic, to isoechoic, and to hypoechoic texture in the submucosa, depending on the EUS probeтs location. This may be due to the differences in the distribution of blood vessels of the lipoma. Gastric angiolipoma on CT shows various degrees of enhancement and heterogeneity in appearance [4], and the general density of the lesion on CT can vary depending on the tissue composition.
Although various imaging modalities could provide some helpful information, the exact method for preoperative diagnosis of gastric angiolipoma is still far away [6,12,13,15]. EUS-guided core needle biopsy could also be a good method for further differential diagnosis of SET lesions such as gastric angiolipoma [16]. However, in our case, due to heterogenic reading on EUS, we determined that partial biopsy would yield different results based on the location of the biopsy on the lesion. For the same reason, we determined that core needle biopsy would not yield the result that is reflective of the lesion as a whole.
The final diagnosis usually depends on histological examination of the excised specimen. Surgical resection is the main treatment option for gastrointestinal angiolipoma, and the recurrence rate is low when the angiolipoma is completely resected. In the reported four cases with bleeding symptoms, the patients were treated with surgical resection [8-11], and the other case was an asymptomatic patient whose fecal occult blood test was identified as weakly positive [3]. Only non-surgical treatment, including proton-pump inhibitors, was performed.
In our case, the patient experienced no specific symptoms, and the lesion showed no ulceration. Regardless, we decided to treat the patient due to his relatively young age and the atypical echogenicity of the lesion during the EUS examination. The lesion size in our case was approximately 4 cm and relatively large; however, it was confined to the submucosal layer on the EUS. Therefore, we performed endoscopic treatment rather than surgical resection. We performed ESD, and the lesion was resected completely. To the best of our knowledge, this is the first case of gastric angiolipoma diagnosed and treated after ESD.
We found a gastric subepithelial lesion in a patient who underwent EGD during a general examination. Because of the unusual features of this lesion, we decided that this lesion should be histologically analyzed. ESD was performed, and the pathologic diagnosis was a gastric angiolipoma.