INTRODUCTION
Endoscopic ultrasound-guided biliary drainage (EUS-BD) is widely used as an alternative treatment for bile duct obstruction after a failed endoscopic retrograde cholangiopancreatography (ERCP) [1]. Some experts use this technique as a first-line drainage modality, given the increasing evidence on its efficacy and safety profile [2,3]. The commonly performed EUS-BD procedures include endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS), endoscopic ultrasound (EUS)-guided choledochoduodenostomy, EUS-guided antegrade approach, and EUS-guided rendezvous technique. EUS-HGS was first described in 2003 and has evolved as a method of internal biliary drainage through the left intrahepatic bile duct for malignant hilar obstruction and benign conditions in patients with a surgically altered anatomy [4-6]. Over the years, its application has extended to right intrahepatic bile duct drainage and dedicated devices have been developed to overcome the technical challenges. This review summarizes the essential practical points, techniques, and equipment available for EUS-HGS.
CASE SELECTION AND SPECIAL PRECAUTIONS
The advantage of the transhepatic approach is the proximity to the left lobe of the liver. The procedure is generally performed in hilar strictures and in cases in which the ampulla is inaccessible, either because of gastric outlet obstruction or a surgically altered anatomy. Careful evaluation of the patientŌĆÖs clinical condition and cross-sectional imaging to check for contraindications are essential, and dilation of the left intrahepatic duct (IHD) is usually required. The following conditions should be considered contraindications or circumstances that warrant special precautions:
ŌĆó Ascites
The presence of ascites is considered a relative contraindication for percutaneous transhepatic biliary drainage because it increases the risk of biliary peritonitis and hematoma [7]. Experts have shown that EUS-HGS can be performed in the presence of some ascites [7,8]; however, stent migration can occur, warranting caution in such patients [9]. Therefore, most authorities suggest that a large amount of ascites is a contraindication for EUS-HGS because it can separate the space between the liver and stomach [10,11]. If the procedure is unequivocally needed, placement of a percutaneous ascites drainage tube is recommended before performing EUS-HGS to prevent complications [12].
ŌĆó Left lobe atrophy
Careful evaluation with cross-sectional imaging before drainage is crucial. Endoscopic drainage of the left IHD in the presence of left lobe atrophy is not suitable and should be avoided.
ŌĆó Tumor infiltration
Tumor infiltration of the gastric wall at the puncture site is a contraindication because of the increased risk of tumor seeding and bleeding [10]. EUS-HGS should be avoided in patients with unresectable gastric cancer with reduced gastric volume because of the increased risk of stent migration [11].
ŌĆó Isolated right intrahepatic bile duct obstruction
Despite the expanding application of EUS-HGS for right IHD drainage, the duodenum is the recommended puncture site for the drainage of isolated right IHD obstruction [13].
STEP-BY-STEP GUIDANCE
Selection of the puncture site is the first crucial step in this procedure. After the puncture of the selected bile duct segment, bile aspiration can be optionally performed. Thereafter, contrast is injected, followed by wire passage. Once the guidewire has been passed through the needle channel and deeply into the desired bile duct, the puncture tract is dilated and a stent can be placed [14]. Recently, many dedicated instruments have been developed to improve the success rate and minimize complications.
Liver segment selection
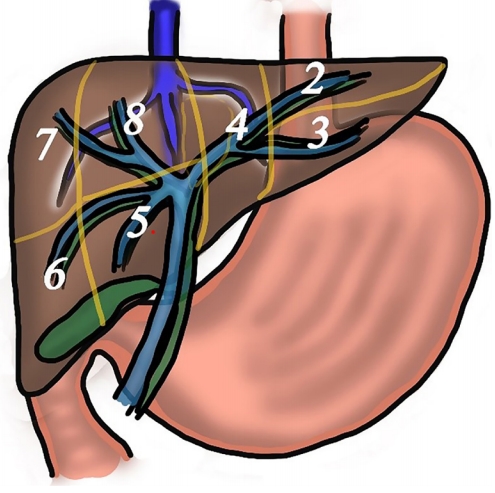
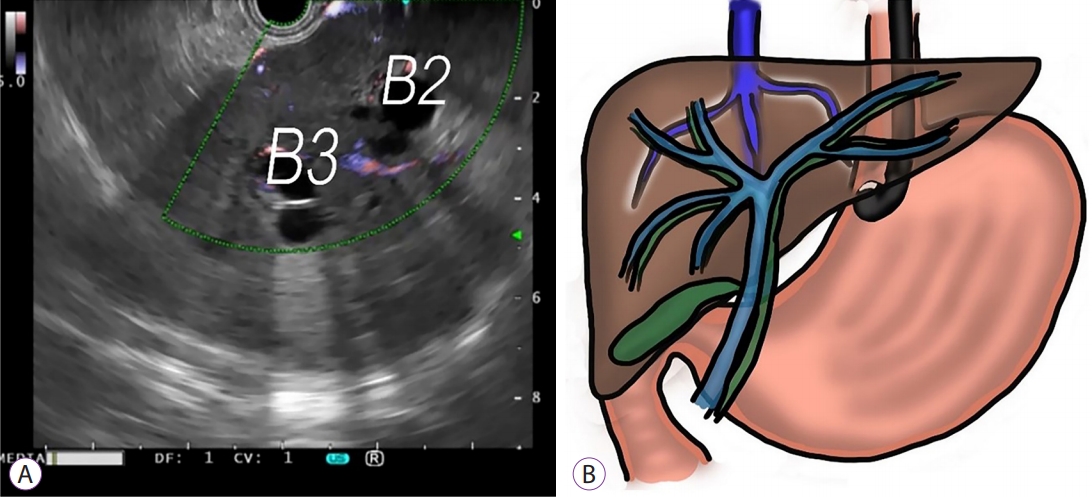
It is important to understand the liver anatomy (Fig. 1) and recognize that segments 2 and 3, located adjacent to the esophagogastric junction, are usually the puncture targets. The selection of the target bile duct and liver segment should be based on many factors, including stricture location, tumor or portal vein invasion, degree of segmental dilatation, and liver atrophy. The left lateral segment is usually visualized when the tip of the echoendoscope is placed at the esophagogastric junction with the scope in the neutral position. Segment 2 is located above, whereas segment 3 is located below, the hepatic vein (Fig. 2) [15]. Although the scope position is straight and guidewire manipulation is easier in segment 2, the puncture site is usually located in the esophagus, increasing the risk of mediastinitis or pneumomediastinum [16]. Thus, puncturing segment 3 is preferred [10]. A hemoclip can be applied at the esophagogastric junction before EUS examination to avoid puncturing through the esophagus [16]. To obtain EUS images of segment 3, the scope is usually pushed down into the gastric cardia with upward angulation toward the liver hilum. Selection of the IHD part is also essential. The size of the IHD is generally larger near the liver hilum, allowing for easier identification; however, placement of a fully covered self-expandable metallic stent (FCSEMS) in the hilar area should be avoided. Ideally, a stent should not block the branches of the IHD, especially in the nonpunctured segment. The technical success rate is higher when the bile duct diameter is >5 mm and the hepatic portion length is 1ŌĆō3 cm [17]. However, the distance of hepatic parenchyma of <2.5 cm is associated with bile leak [18].
Scope position
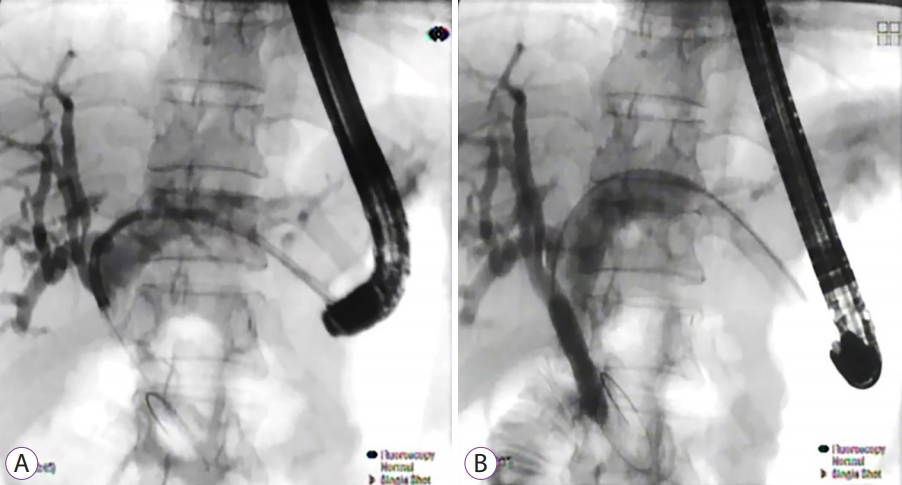
The echoendoscope is usually placed in a short position with upward angulation toward the lesser curvature of the gastric cardia when performing EUS-HGS. The scope position and the needle direction are essential considerations for successful guidewire manipulation; therefore, adjusting the scope position under fluoroscopy guidance is recommended before starting the procedure. An obtuse angle between the scope and the needle helps increase the success rate of guidewire insertion [19]. However, the forward force during instrument insertion may be reduced when the scope is in an angulated position, resulting in looping and displacement of the equipment (Fig. 3). Another technique that has been proposed to improve the stability of the scope during the procedure is inserting a second guidewire adjacent to the first wire. This technique helps fix the scope to the tract, improves guidewire visibility on EUS, and provides a rescue wire in case of technical failure [20].
Needle preparation
A 19-G needle is required for puncture and wire insertion. Before the procedure, the stylet is usually removed and the needle is primed with saline or contrast to eliminate entry of air into the bile duct. A specially designed needle has been made for EUS intervention, with a sharp stylet tip and blunt needle end to minimize wire shearing during the procedure [21]. In a nondilated intrahepatic bile duct and when a 19-G needle is too large, a 22-G needle with a 0.018- or 0.021-inch guidewire may be considered.
Guidewire selection
A stiff wire with a flexible tip is an appropriate guidewire for interventional EUS. Although a 0.035-inch guidewire is small enough to pass through a 19-G needle, it shears easily and can be challenging to manipulate because of its size. Some authors recommend using a hydrophilic 0.035-inch guidewire without coating to reduce the chance of wire shearing [8]; however, a stiff 0.025-inch guidewire is preferable [10]. When a 22-G aspiration needle is used to puncture the bile duct, only a stiff 0.021- or 0.018-inch guidewire can be inserted. A successful EUS-guided rendezvous using a 22-G needle and a 0.018-inch guidewire has been reported [22]. The development of a 0.018-inch stiff guidewire allows instrument insertion without the need for wire exchange [23,24].
Tract dilation
The two main types of dilation equipment are cautery and mechanical dilators. A cautery-type dilator, known as a needle- knife, has been used in earlier studies [25]. The needle-knife is often in a tangential orientation when it is inserted over an angulated scope, resulting in undesirable cuts and increased risk of complications [26]. Currently, the coaxial electrocautery dilator has replaced the needle-knife cautery dilator [11]. The electrocautery device is beneficial in patients with a fibrotic liver; however, more bleeding is observed in such cases [27], raising concerns about an ŌĆ£overburningŌĆØ effect [24]. In terms of the mechanical dilator, the two most commonly used equipment are the balloon dilator and the dilation catheter [24,28]. The drawback of multistep tract dilation is the risk of bile leakage during the procedure. Therefore, a new dilation tool has been developed to facilitate tract creation, dilation, and stent insertion without instrument exchange. This ŌĆ£all-in-oneŌĆØ equipment includes the 3-Fr tip balloon catheter (REN biliary dilation catheter; KANEKA, Osaka, Japan) [29,30], combined 4-Fr tip balloon catheter with a stylet for tract dilation [31], a metallic stent with a thin delivery system [32], or a metallic stent with electrocautery at the tip of the delivery system [33]. The specially designed tract dilation devices are summarized in Table 1.
Stent selection
Although both straight plastic stents and fully covered self-expandable metallic stents (FCSEMS) have been conventionally used, plastic stents are known to have the disadvantages such as stent occlusion and bile leakage, especially with large-tract dilation. Meanwhile, FCSEMS has gained popularity because it provides a larger drainage diameter through a small endoscopic channel; however, it has drawbacks such as stent migration and potential blockage of the IHD side branches. Recently, a dedicated plastic stent for interventional EUS has been developed [35]. This newly designed plastic stent has a single pigtail with a tapered tip and four flanges to prevent migration. In addition, it has a small diameter, which might reduce the risk of IHD blockage. Nevertheless, this type of stent is not widely available outside Japan and periodically requires stent exchange. Furthermore, a dedicated partially covered self-expandable metallic stent (PCSEMS) with an antimigration design has been released. This stent has an uncovered portion for the IHD part to prevent blockage of small branches, as well as a fully covered portion for the area between the liver and gastric wall to prevent bile leakage, with a flared end in the stomach side preventing inward migration [36,37]. Some experts prefer a 6-mm FCSEMS to reduce the chance of IHD blockage and biliary hyperplasia, which can occur with a large-bore metallic stent. However, stent dysfunction and dislocation have been reported in up to 50% of cases [38].
COMPLICATIONS AND TROUBLESHOOTING
Vascular injury from needle puncture
Portal vein and hepatic artery injuries can cause immediate or delayed bleeding. Bleeding from a hepatic artery pseudoaneurysm after EUS-HGS has been reported, with all patients successfully treated with transarterial interventions [39,40]. If a vascular structure is accidentally punctured, bleeding can be prevented by retracting the needle until the tip is in the liver parenchyma, followed by reinsertion of the stylet to push back the retained clot inside the needle to occlude the puncture tract.
Guidewire problems
Shearing can occur when the guidewire is shaved by the needle tip during manipulation, especially if the angle between the guidewire and the needle is acute [41]. Gentle guidewire retraction, exchanging the needle to a catheter before guidewire manipulation [42], and using a blunt needle tip with a sharp stylet (Cook Medical; Bloomington, IN, USA) [43] have been proposed to minimize this problem. If shearing occurs, forward guidewire insertion and slight retraction to keep the needle tip inside the liver parenchyma, so-called liver impaction technique, has been reported [44]. Recently, a steerable access needle device (18.5-G, 90┬░, Beacon EUS access system; Covidien; St Louis, MO, USA) has been developed to avoid wire shearing during manipulation [45,46].
Furthermore, coiling and incidental advancement of the guidewire toward the peripheral bile duct often occur during manipulation. In these circumstances, the needle can be removed and replaced by an ERCP cannula or coaxial dilator to aid guidewire manipulation.
Bile leak
Bile leak after EUS-HGS is not unusual. Factors associated with bile leak include use of a needle knife, noncoaxial electrocautery, and plastic stent placement [26,47]. A retrospective study reported that the number of punctures (>1), procedure time (>20 min), distance to the liver parenchyma (<2.50 cm), and presence of acute cholangitis were significantly associated with bile peritonitis; however, only short distance to the liver parenchyma (<2.5 cm) remained significant in multivariate analysis. Most patients in the study underwent tract dilation using a noncautery method [18]. The use of a covered metal stent in the distal part between the liver and the gastric wall is recommended to prevent bile leak [1]. Thus, a newly developed equipment that reduces instrument exchange and procedure time might reduce bile peritonitis.
Stent migration
Stent migration is one of the most severe complications associated with mortality [48-50]. It can occur immediately or a few days after the procedure [48,49,51,52]. Thus, the technique of stent deployment is important. Inadequate traction of the stent during deployment may lead to a long gap between the liver and the outer gastric wall, causing stent trapping between these two structures, described as a ŌĆ£candy signŌĆØ (Fig. 4) [53]. Therefore, sufficient tension should be applied during the opening of the stent to avoid this problem. Generally, intrascope channel stent deployment is recommended [31,53]. In addition, a stent length on the gastric side of >3 cm is advisable [54].
If stent misplacement occurs during deployment, rescue maneuvers can be performed while leaving the wire in place and placing another stent in tandem fashion [52]. Repositioning of the migrated metal hepaticogastrostomy stent using foreign- body forceps and placing an additional stent [51,55], as well as EUS-guided puncture through the gastric opening and placement of another metallic stent have been described [50]. If bile leak continues, converting the biliary passage from the HGS site to either a transpapillary [9] or percutaneous route may be required [49].
Many preventive measures have been proposed to prevent delayed stent migration, including using a longer stent or a partially covered self-expandable metallic stents [56], insertion of a double pigtail stent inside the metallic stent [42], using a plastic stent as an anchor to keep the metallic stent in place [51], and using a combination of uncovered and covered stents to lock the intrahepatic portion [57].
OUTCOMES AND APPLICATION
The technical success rate has increased to 90ŌĆō100% with refinements in equipment and techniques [47,58]. Recurrent biliary obstruction can occur 5.5ŌĆō8.5 months after the procedure [37,56,58]. EUS-HGS is primarily performed for malignant obstruction. Recently, it has been used for anastomotic strictures in patients with a surgically altered anatomy [5,59] (Fig. 5) and as a portal for direct cholangioscopic-guided lithotripsy of IHD stones [60-62]. Lithotripsy via the hepaticogastrostomy tract can be safely performed 1ŌĆō4 weeks after the initial procedure [60,61]. The technical success rate for benign conditions is similar to that for malignant obstruction, but stent dysfunction occurs frequently when metallic stents are used. Therefore, they should be changed for plastic stents in a scheduled manner; however, the reintervention rate is high because of stent dysfunction [59]. Data on long-term outcomes in benign conditions are still lacking.
In the future, one-step EUS-HGS can be achieved using a novel dedicated device with the development of a cautery tapered-metal-tip delivery system [33]. Device refinement can improve technical success and minimize complications.
CONCLUSIONS
This review provides a summary of technical tips and information on currently available devices for EUS-HGS. Adverse events can be avoided with proper case selection, good understanding, and adequate technical skills during each step. Early recognition of complications and performing troubleshooting are essential for a successful procedure. Finally, a dedicated device is needed to simplify the procedure, improve the success rate, and reduce complications.