CME for
KSGE members
Taki, Maekita, and Kitano: A Rare Case of a White-Furred Ileocecal Valve
Quiz
A 33-year-old, homosexual, sexually active man presented to the hospital with anal pain and hematochezia for >1 month. He had no signs of diarrhea or fever and no significant medical or pharmacotherapeutic history. Laboratory blood examination revealed increased white blood cell count (10,080; reference, 3300ŌĆō8600/┬ĄL), C-reactive protein level (11.0; reference, 0.00ŌĆō0.14 mg/mL), squamous cell carcinoma antigen (7.2; reference, 0ŌĆō1.5 ng/mL), and HBs antigen (1067; reference, <0.005 IU/mL). Serum carcinoembryonic antigen (2.8; reference, 0ŌĆō5 ng/mL), carbohydrate antigen 19-9 (17.3; reference, Ōēż37 U/mL), and cytomegalovirus antigenemia assay (C7-HRP) were all within reference ranges. No abnormalities were observed in the blood or fecal cultures. Computed tomography showed wall thickening from the left anus to the rectum. Colonoscopy showed a white-furred ileocecal valve, edematous and rough-surfaced mucosa throughout the entire colon, and an irregular and deep rectal ulcer ( Fig. 1). Biopsy specimens were collected from every part of the colon and the ileocecal region. What is the diagnosis of a white-furred ulcerative lesion in the colon?
Answer 
Syphilitic colitis coinfected with human immunodeficiency virus (HIV): However, other causes of ulcerative lesions, such as anal or rectal ulcers, inflammatory bowel disease, malignant disease, and other sexually transmitted diseases (cytomegalovirus, Neisseria gonorrhoeae infections, lymphogranuloma venereum, etc.) should also be considered. In addition, ileocecal ulcer requires exclusion of intestinal tuberculosis, CrohnŌĆÖs disease, intestinal BehcetŌĆÖs disease, and infectious enteritis. In the present case, blood examinations confirmed Treponema pallidum hemagglutination, rapid plasma reagin, and HIV test results were positive. Histopathological examination showed Treponema pallidum immunostaining ( Fig. 2A); therefore, the patient was diagnosed with syphilitic colitis and anal canal cancer. No other symptoms of syphilis infection were observed. The ulcer showed a tendency to improve after an intravenous administration of ceftriaxone sodium hydrate at 1 g/day for 1 week ( Figs. 2B, 2C). Therefore, the patient was finally administered antibiotics for 5 weeks. After controlling for syphilis infection, chemoradiotherapy for anal canal cancer and highly active antiretroviral therapy for HIV were initiated. The syphilis infection rate tends to be high among patients with HIV [ 1]. Rapid progression to more advanced stages and a higher risk of treatment failure have been reported for syphilitic colitis in HIV-coinfected patients [ 2]. Syphilitic colitis is often missed, owing to the wide variety of clinical presentations. Endoscopic findings of syphilitic colitis are commonly observed as single or multiple furred ulcerative lesions in the anterior wall of the lower rectum, further mass formation, and luminal stenosis. In the present case, the ring-shaped fur surrounding the ileocecal valve revealed second-stage syphilis due to bloodstream infection. Anal canal cancer, syphilitic proctitis, and HIV-infection complications occurred; however, the relationship among these symptoms has not been clarified. In conclusion, deep ulcerative lesions of the anus and atypical colitis should be considered to potentially be associated with anal cancer and syphilitic enteritis in HIV-infected individuals.
Fig.┬Ā1.
Colonoscopy examination. (A) Colonoscopy showed a white-furred ileocecal valve. (B) Edematous and rough-surfaced mucosa throughout the entire colon. (C) Irregular and deep rectal ulcer. 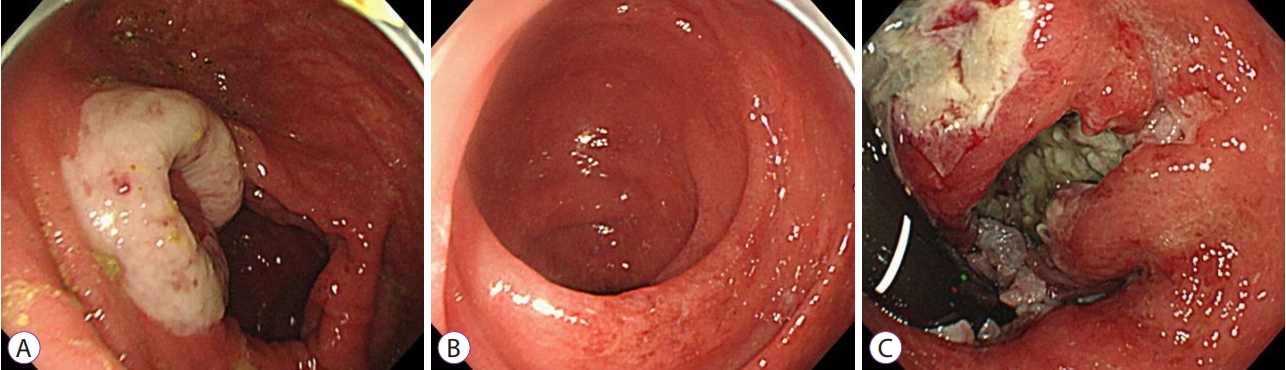
Fig.┬Ā2.
Histopathological and colonoscopy examinations. (A) Histopathological examination showed Treponema pallidum on immunostaining. (B, C) Colonoscopy showed that the ulcer showed a tendency to improve after an intravenous administration of ceftriaxone sodium hydrate at 1 g/day for 1 week. 
REFERENCES
1. Chen SY, Gibson S, Katz MH, et al. Continuing increases in sexual risk behavior and sexually transmitted diseases among men who have sex with men: San Francisco, Calif, 1999-2001, USA. Am J Public Health 2002;92:1387ŌĆō1388.  2. Ghanem KG. Evaluation and management of syphilis in the HIV-infected patient. Curr Infect Dis Rep 2010;12:140ŌĆō146. 
|
|







