INTRODUCTION
Endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) was first prescribed as a rescue technique following failed drainage by endoscopic retrograde cholangiopancreatography (ERCP).1,2 However, recently, indications EUS-HGS include difficult ERCP cases, and now it is even being performed for primary drainage.3 EUS-HGS through duct B3 is a widely accepted technique because it has a larger diameter, and the puncture can be performed safely via the trans-gastric approach.4
EUS-HGS through duct B2 has been reported by Hara et al.5 using forward-viewing EUS with an ultraslim needle and guide wire. In most patients, B2 directly joins B3; therefore, either of B3 or B2 routes are adequate for decompression of biliary obstruction. However, in some patients, these two ducts do not join together, and thus, single-route drainage is not sufficient.
Here, we report our experience of performing EUS-HGS via both B2 and B3 simultaneously in patients in whom B2 and B3 were divided.
CASE REPORT
We reviewed cases from the Department of Gastroenterology, Aichi Cancer Center, between February 2019 and April 2021. We retrospectively examined seven patients (median age, 63 years; range, 41ŌĆō77 years), (four men and three women) in whom B2 and B3 were divided by invasive hilar tumor. EUS-HGS using both B2 and B3 was performed during the same session. Our rationale for performing EUS-HGS by puncturing both B2 and B3 was to effectively treat biliary obstruction in patients with divided B2 and B3.
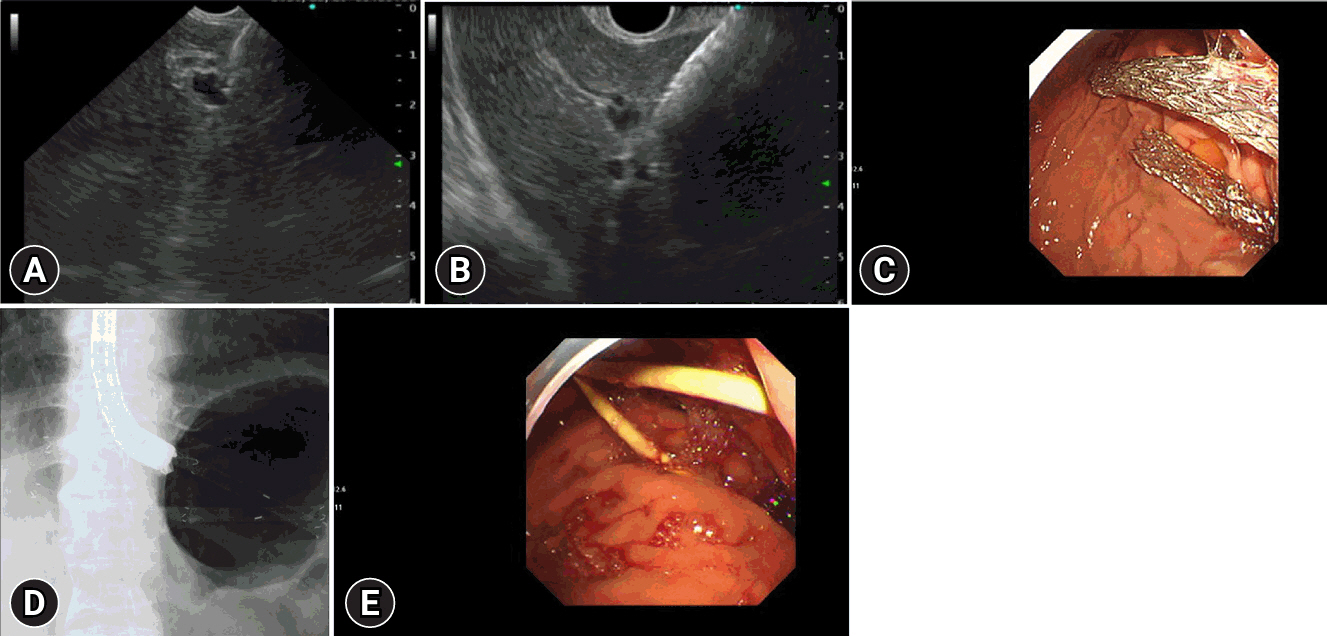
EUS-HGS was performed by a skilled endoscopist at our center. EUS was performed using both oblique-view EUS (OV-EUS, UCT260; Olympus Co., Tokyo and 580UT; FUJIFILM Co., Tokyo, Japan) and forward-view EUS (TGF-UC180J; Olympus Co., Tokyo, Japan). First, the cardia was marked using an endoclip to identify the EG junction under fluoroscopy to avoid inadvertent transesophageal puncture. Second, both B2 and B3 were confirmed by color-Doppler imaging to avoid vessel puncture, and the duct was then punctured by either a 19-G or 22-G needle preloaded with a 0.018-inch guidewire or 0.025-inch guidewire (Fig. 1A, B). Third, the bile duct was confirmed by observing the wire direction and contrast medium. The fistula was gradually dilated using a dilator catheter (ES dilator; Zeon Medical, Tokyo, Japan) and Tandem XL Triple Lumen ERCP Cannula (Boston Scientific, Tokyo, Japan). Some patients required additional balloon dilation of the fistulas. Notably, none of the patients required electrocautery-dilation.6,7 Finally, we deployed an FCSEMS (6mm├Ś12 cm or 15 cm, Niti-S biliary S-type stent, TaeWoong Medical Co,.LTD, Gimpo, Korea; Hanarostent, M.I. TECH, Gyeonggi-do, Korea) in five patients (Fig. 1C, D).
We used a 7F plastic stent in two patients (Flexima Biliary Stent, Boston Scientific; type IT stent Gadelius Medical K.K., Tokyo, Japan) (Fig. 1E).
Computed tomography was performed in all patients, 24 hours after the procedure, to assess adverse events, such as stent migration and bile leakage.
Table 1 illustrates the patient characteristics, Table 2 shows the details of the procedure and devices, and Table 3 shows the outcomes of the procedure and adverse effects.
Here, we report a 100% technical and overall clinical success rate. Technical success is defined as the ability to complete such a procedure safely without significant adverse effects, while clinical success is defined as the relief or substantial reduction of preprocedural symptoms, such as jaundice and fever. Early adverse effects were closely monitored. Minimal bleeding in one patient (1/7) and mild peritonitis in one patient (1/7) were observed. No patient showed evidence of stent dysfunction or dislocation on follow-up CT. None of the patients developed fever or bile leakage after the procedure.
DISCUSSION
There are many anatomical variations in the confluence of the left hepatic duct. In the majority of cases, B2 and B3 are directly connected to each other such that drainage of one of them is sufficient for adequate biliary drainage. However, in some cases, B2 and B3 are divided either by tumor invasion or by normal anatomical variation, which makes the drainage of both ducts necessary for effective drainage.8
In this study, we reported the efficacy and safety of performing EUS-HGS through both B2 and B3 separately during the same session in patients in whom B2 and B3 were divided. The most important points to be considered in this new intervention are technical success, clinical success, and safety. We performed EUS-HGS in seven patients, by puncturing both B2 and B3, with 100% technical and overall clinical success rates.
The management of hilar obstructive jaundice is both difficult and complicated. The placement of multiple metal stents is effective in some patients for a limited duration. However, re-intervention in situations involving multiple stents is usually difficult. Multiple plastic stents are also effective (stent-by-stent), but three plastic stents are typically most frequently deployed via a trans-papilla approach. Our suggestion is to drain the right lobe using 2 to 3 trans-papillary plastic stents and to perform two EUS-HGSs to drain the left lobe through B2 and B3. To the best of our knowledge, our study is the first to describe EUS-HGS through both the B2 and B3 routes simultaneously. The B3 route is the most widely recommended route for EUS-HGS because of the wider caliber of B3 and no intervening branch of the portal vein. Moreover, B3 is deeper than B2; therefore, the puncture is always via the lesser curve of the stomach. However, guidewire negotiation, dilation, and stent deployment are more difficult because of the angled course of B3.9
B2-puncture is an easier approach for the rendezvous technique because of the direct continuation between B2 and the left hepatic duct. However, B2-puncture using OV-EUS sometimes inadvertently takes a transesophageal route; therefore, we usually use forward-viewing EUS for B2-puncture and apply up-angulation while scoping in the stomach for better visualization and puncturing B2 from the lesser curve of the stomach.5,10
Theoretically, puncturing both B2 and B3 during the same session increases the risk of complications. However, we experienced minimal side effects in the form of minor bleeding and mild peritonitis. The bleeding observed in the patient was due to tumor invasion and not a complication of the procedure. It was self-limited and managed effectively using an endoclip. The patient who developed mild peritonitis had preexisting ascites, which increased the risk of peritonitis.
Our team has previously reported the superiority of using 6 mm, 12 cm FCSEMS for EUS-HGS. A smaller caliber reduces the risk of focal cholangitis, while a longer stent better resists stent migration. Deploying fully covered stents in this intervention enables stent exchange and re-interventions.3 However, we deployed plastic stents in two patients in this study because B2 and B3 were not dilated. We prefer and recommend placing plastic stents to prevent focal cholangitis.
Our study has some limitations. First, this was a small cohort study. Second, the retrospective nature of the study may have introduced a selection bias. Third, this study was conducted at a single center. Therefore, a multicenter study is needed to examine this technique.
We conclude that EUS-HGS through both B2 and B3 during the same procedure is safe, feasible, and effective for biliary drainage in patients with divided B2 and B3. Careful patient selection for this procedure is recommended to achieve better outcomes. Patients with ascites may be at risk for peritonitis and may benefit from therapeutic paracentesis prior to the procedure. This procedure should be performed by experienced, skilled endosonographers to minimize procedural time and decrease the risk of side effects.