INTRODUCTION
Endoscopic procedures requiring repeated endoscope insertion are painful for the patient and difficult for the endoscopist.1 Recently, overtubes, such as the Guardus overtube (US Endoscopy Group Inc.), which makes repeated endoscope insertion easier, have been produced for endoscopic procedures. However, fatal complications, such as intestinal perforation and pain associated with breakage of the rigid overtube material, can occur with overtube use.2-6 Moreover, most overtubes have shallow insertional depths; therefore, inserting them into the distal portions of the intestinal tract, such as the cecum, is difficult.
In a previous study, we developed a guide tube that compensates for the disadvantages of rigid overtubes.1 The guide tube was a soft silicone overtube. Various endoscopic procedures using a guide tube have been performed in a gastrointestinal simulator.1 We observed that all guide tube-assisted endoscopic procedures were safer and more effective than conventional endoscopic techniques when performed using gastrointestinal simulators. However, because the gastrointestinal simulator does not produce peristaltic gastrointestinal movement, and the gastric and colonic lumens of the simulator are made of silicone, evaluating the risk of mucosal perforation using this test model was difficult. Therefore, in this study, we used an in vivo porcine model to overcome these limitations and evaluate the clinical outcomes of guide tube use.
METHODS
Statement of animal ethics and animal care
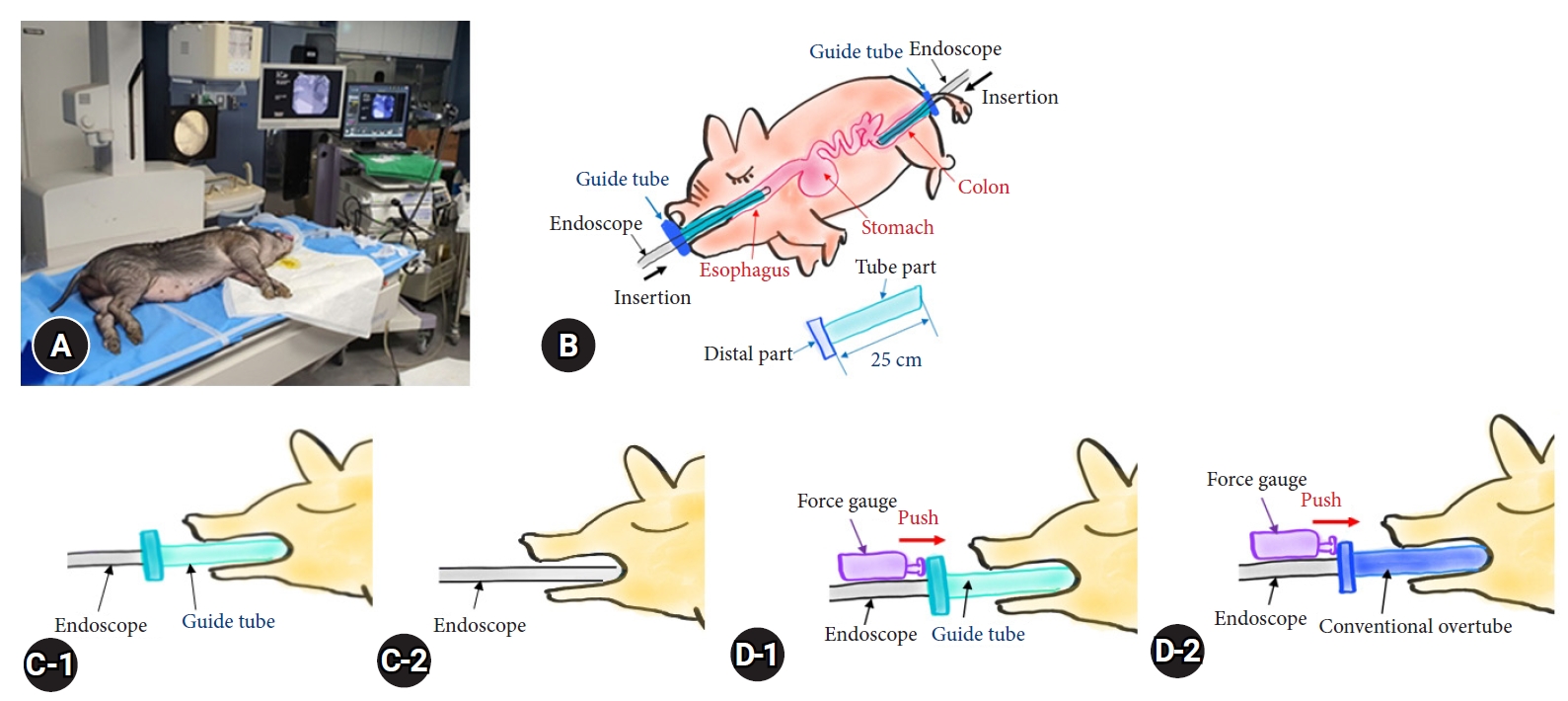
This study was a preclinical trial performed in July 2019 using a 14-month-old pig weighing 32 kg as the in vivo porcine model for all tests (Fig. 1). Experiments were performed according to the regulations and guidelines provided by the committee. The description of this study follows the Animal Research: Reporting of In Vivo Experiments guidelines. The pig underwent fasting and intestinal cleansing a day before the procedure. On the day of the procedure, the animal was sedated with atropine sulfate (0.4 mg/kg) and xylene (2 mg/kg) and was then anesthetized through inhalation of 0.5% isoflurane. The target lesions for the endoscopic procedures were generated artificially as part of the porcine model. Two endoscopists from the SMG-SNU Boramae Medical Center, Seoul, Korea, participated in the study. The animal was sacrificed after the experiment according to the IACUC guidelines.
Devices and settings
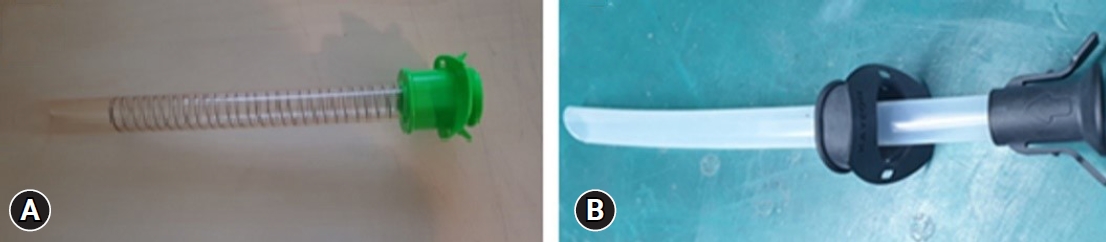
In this study, we used a single-channel endoscope (GIF-Q260J; Olympus Co., Ltd.) for manipulation. Argon plasma coagulation (Olympus Co., Ltd.) and electrocauterization (VIO 300D; ERBE) were used to create the lesions. An insulation-tipped knife-2 (Olympus Co., Ltd.) was used for the lesion resection and submucosal dissection. A guide tube (SMG-SNU Boramae Medical Center; inner diameter, 13 mm; outer diameter, 15 mm; length, 25 cm) was used in the experimental tests. A conventional overtube (Sumitomo Bakelite Inc.; inner diameter: 15 mm; outer diameter: 18 mm) was used in the control tests (Fig. 2). A digital force gauge (ARTBULL) was used to measure insertion force.
Outcomes and data analysis
1) Efficacy evaluation of the guide tube
The primary measurement of outcome efficacy was the approach time(s) of endoscope insertion, defined as the time required to advance the endoscope from the upper incisors to the target sites, such as the esophagus, antrum, and sigmoid colon. Approach times were measured with a stopwatch in two groups as follows: a guide tube group, in which the endoscope was inserted into the target lesion through the guide tube (Fig. 1, C-1), and a control group, in which the endoscope was inserted into the target lesion without a guide tube (Fig. 1, C-2).
Several techniques for improving efficacy have been tested using a guide tube. Multiple foreign body extractions (pork meat: 10 pieces, each measuring 2 cm in diameter), multiple polypectomies (stomach and colon polyps: three each, each measuring 1 cm in diameter), and multiple submucosal dissections (gastric lesions: three, each measuring 2.5 cm in diameter) were performed using the guide tube. Procedure time was not measured in any of the above mentioned procedures.
Safety evaluation of the guide tube
The primary measurement of safety outcome was the insertion force required for guide tube insertion. We selected the proximal esophagus, an area where mucosal perforation frequently occurs during the insertion of an overtube, as the site for assessing the resistance experienced during insertion of each tube. To measure the insertion force, we pushed the distal part of the overtube using a force gauge (SF-100; digital force gauge). The insertion force (kgf) was measured in two groups: the guide tube group, in which the guide tube was inserted into the proximal esophagus (Fig. 1, D-1), and the control group, in which a conventional overtube was inserted into the proximal esophagus (Fig. 1, D-2). The force of insertion in the sigmoid colon was not measured. Radiographs were checked to locate the perforations 3 hours after the guide was inserted into the esophagus and sigmoid colon 50 times for each time.
RESULTS
Efficacy evaluation
The efficacy of the guide tube for endoscopy was demonstrated using an in vivo porcine model. Compared to the conventional endoscopic approach, the guide tube-assisted endoscopic approach had a shorter approach time to reach the distal esophagus (3.35┬▒0.38 seconds and 7.90┬▒0.74 seconds, respectively, p<0.001), antrum (6.16┬▒0.62 seconds and 20.60┬▒2.59 seconds, respectively, p<0.001), and sigmoid colon (2.95┬▒0.43 seconds and 8.15┬▒0.75 seconds, respectively, p<0.001) (Table 1).
Multiple foreign body extractions, polypectomies, and submucosal lesion dissections were successfully performed. A guide tube was used to remove multiple foreign bodies (pork meat: 10 pieces, each measuring 2 cm in diameter), perform multiple snare polypectomies (stomach and colon polyps: three of each, measuring 1 cm in diameter), and perform multiple submucosal dissections (gastric lesions: three, measuring 2.5 cm in diameter) (Fig. 3).
Safety evaluation
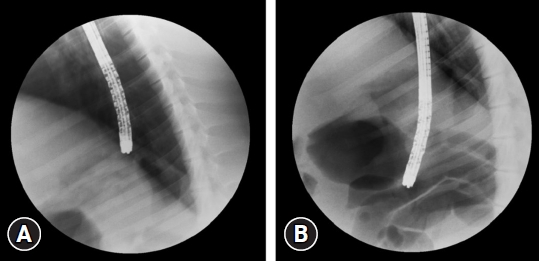
Less resistance was encountered during the insertion of the guide tube into the upper esophagus compared to the resistance measured during the insertion of the conventional overtube (0.96┬▒0.10 kg and 1.49┬▒0.09 kg, p<0.001) (Table 2). Perforation was not observed on follow-up radiographs obtained 3 hours after the guide tube was inserted 50 times for each time in the esophagus and sigmoid colon (Fig. 4).
DISCUSSION
Endoscopic procedures performed using current endoscopic platforms are limited by the narrow and complex gastrointestinal tract. Only small objects can be removed through an endoscope channel with a diameter of <3.2 mm. Therefore, repeated endoscopic insertion is required to remove multiple large polyps or foreign bodies.7,8 Repeated endoscopic insertions are difficult for both patients and endoscopists. Several overtube devices have been designed to facilitate endoscopy.6,9,10 However, the use of overtubes is limited owing to complications such as pharyngeal and esophageal perforations, pneumomediastinum, variceal rupture, and tracheal compression. Recently, a novel shape-locking overtube (ShapeLock) was developed to facilitate repeated endoscopic insertions.11,12 However, the prohibitive cost and complexity of the device limits its use.
The guide tube was made of silicone and named based on its proposed use to provide a guided path to various gastrointestinal lesions during endoscopy procedures. The silicone fabrication of the guide tube reduces the mucosal trauma caused by the rigid materials used to make conventional overtubes. The guide tube is useful in difficult gastrointestinal endoscopic procedures. It can be used to remove large, sharp foreign bodies such as fish bones, blades, or mussel shells; can be easily adapted for use with specialized procedures such as repetitive endoscopic submucosal dissections or endoscopic mucosal dissections of multiple large polyps; and provides a pathway for endoscopic drainage of bulk food material or blood for patients with gastroparesis or gastrointestinal bleeding.
The development and experimentation with endoscopic accessory devices are essential for advancing the diagnosis and treatment of gastrointestinal disorders. This preclinical trial aimed to evaluate the efficacy of the guide tube as an endoscopic accessory device for improving the accessibility of gastric lesions. To minimize animal use in the evaluation of the guide tube, we used a human simulator device for testing in a previous study.1 In the current study, we performed various experiments in a short period without complications using only one pig. Endoscopic procedures that required repeated endoscopic access were performed faster, easier, and safer with the guide tube-assistive device than with a conventional endoscopic overtube. Compared to the conventional endoscopic method, all endoscopic procedures performed with the guide tube had shorter approach times and encountered lower resistance to endoscope advancement. Multiple foreign body extractions, polypectomies, and submucosal dissections were easily performed using guide tube-assisted endoscopy. Furthermore, mucosal perforation did not occur during any of the guide tube-assisted procedures.
This study has several limitations. First, it was a single-center, preliminary study based on few swine experiments. Nevertheless, this experimental bias was minimized by conducting several pretests using realistic animal model simulators. Second, due to the anatomical differences between the porcine and human gastrointestinal systems, the guide tube-assisted endoscopy results may not be the same for human patients as they were for the animal used in this preclinical study. Therefore, long-term evaluation of this endoscopic technique in human patients is needed. Lastly, the time required for efficacy-related procedures, such as multiple foreign body extractions, polypectomies, and submucosal lesion dissections, was not measured because of limited research funding.
In conclusion, this study was designed to test the efficacy and safety of endoscopy using a guide tube. Despite the limitations of this study, our results demonstrated that guide tube-assisted endoscopy was effective and safe for performing procedures requiring repeated endoscopic access in an in vivo porcine model. Large-scale human studies are required for further clinical implementation.