Predicting Colonoscopy Time: A Quality Improvement Initiative
Article information
Abstract
Background/Aims
There is lack of consensus on the optimal time allotted for colonoscopy, which increases patient wait times. Our aim was to identify and quantify the individual pre-procedural factors that determine the total procedure time (TPT) of colonoscopy.
Methods
This retrospective study involved 4,494 subjects, undergoing outpatient colonoscopy. Effects of age, sex, body mass index, abdominal surgery history, procedure indication (screening, surveillance, or diagnostic), procedure session (morning or afternoon), and endoscopist’s experience (fellow or attending) on TPT were evaluated using multiple regression analysis. A p<0.05 was considered significant.
Results
A total of 1,239 subjects satisfied the inclusion/exclusion criteria. Women, older individuals, and those with a history of abdominal surgery were found to have a shorter TPT (p>0.05) as did afternoon session colonoscopies (p=0.004). Less experienced endoscopists had longer TPTs (p>0.05). Screening (p=0.01) and surveillance (p=0.008) colonoscopies had a longer TPT than diagnostic procedures. Overall, the F-value of the regression model was 0.0009.
Conclusions
The indication for colonoscopy and the time of day have statistically significant associations with TPT. These results will help in streamlining workflow, reduce wait time, and improve patient satisfaction.
INTRODUCTION
Colorectal cancer (CRC) is one of the leading causes of malignant neoplasm-related mortality [1,2]. In 2012, CRC was responsible for 694,000 deaths worldwide, accounting for 8.5% of all cancer-related deaths [2]. It is estimated that in the United States alone, 93,090 new cases of CRC will be diagnosed in 2015 [3]. Despite the surge of newer CRC screening tests, colonoscopy has continued to be the gold standard. It is not only a screening modality but also a diagnostic and interventional tool. Vijan et al. [4] developed a decision model that estimated that approximately 4.5 million colonoscopies would be performed annually in the United States if 100% of age-eligible subjects (older than 50 years) are screened with colonoscopy.
The time needed to perform a colonoscopy depends on characteristics of both the patient and the endoscopist. A colonoscopy has two components, the cecum intubation and the withdrawal. “Difficult colonoscopy” is a term used to describe cases that require longer than usual to achieve cecum intubation. The endoscopist’s level of training, quality of bowel preparation, scheduled time for the procedure (morning vs. afternoon), body habitus, age, sex, intra-abdominal adhesions secondary to previous surgery, and presence of angulations among the large bowel loops predict the level of difficulty in achieving cecum intubation [5,6].
The American Society of Gastrointestinal Endoscopy recommends a minimum withdrawal time of 6 minutes in screening colonoscopy with negative findings to assure the quality of procedure [7], but the factors affecting withdrawal time are not well-defined in the literature. By extrapolating our knowledge from factors affecting cecum intubation, we postulate that endoscopist’s experience, bowel preparation quality, indication for colonoscopy, and types of interventions (e.g., polyp removal, mucosal biopsy) are probably the key drivers of withdrawal time during colonoscopy.
At present, even though we know that all colonoscopies are not the same, when it comes to scheduling the procedure in the endoscopy suite there is no distinction concerning the time allotted for each colonoscopy. This results in increased patient waiting time, higher patient dissatisfaction, and poor patient follow-up.
All of the factors affecting colonoscopy are known at the time of scheduling the procedure (other than whether an intervention will be necessary and the bowel preparation quality). We designed our retrospective study to identify and quantify the various pre-procedural factors in order to determine a way to predict the total procedure time (TPT) necessary for a colonoscopy.
MATERIALS AND METHODS
Study objective
To identify and quantify the effect individual pre-procedural factors have on the TPT for colonoscopy.
Study design
This was a retrospective observational cohort study done at a tertiary care teaching hospital. The study was approved by our Institutional Review Board (IRB ID 4550EXE approved on 12/16/13). Written informed consent was waived due to the study’s retrospective nature.
Study population
Inclusion criteria
All subjects presenting for an outpatient colonoscopy at our institution over a span of 18 months.
Exclusion criteria
Subjects with poor bowel preparation, failure of cecum intubation, incomplete data, any intervention during the colonoscopy (e.g., biopsy or polyp removal), personal history of colectomy, personal history of inflammatory bowel disease (IBD), or personal or family history of CRC.
Study methods
The colonoscopy and anesthesia procedure reports were reviewed to collect data regarding age, sex, weight, height, past medical history (of IBD and CRC), past surgical history (colectomy or any other abdominal-pelvic surgery, including laparoscopic procedures but not umbilical/inguinal hernia repair and transurethral/transvaginal procedures), family history of CRC, indication for the colonoscopy (screening, surveillance, or diagnostic), bowel preparation quality, timing of the procedure (morning or afternoon), endoscopist’s experience (fellow or attending), interventions during the colonoscopy (biopsy or polyp removal), and TPT. The exclusion criteria were then applied to the initial study population to remove the effects of the confounding variables. Weight and height were then used to calculate body mass index (BMI). All of the data were recorded on Excel spreadsheets (Microsoft, Redmond, WA, USA) without including any identifying information to maintain anonymity.
The effects of the seven variables (age, sex, BMI, abdominal surgery history, procedure indication [screening, surveillance, or diagnostic], timing of the procedure [morning or afternoon], and endoscopist’s experience [fellow or attending]) on TPT was evaluated using a multiple regression analysis model. A p<0.05 was considered to be statistically significant.
RESULTS
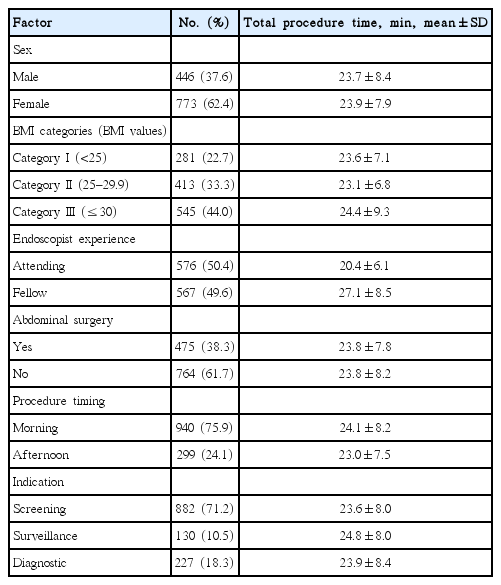
A total of 1,239 subjects with a mean age of 57.9 years satisfied the exclusion criteria. The demographic characteristics of the study population are described in Table 1. It was composed of 62.4% women and 37.6% men. The distribution of cases across the day was non-uniform with 75.9% procedures performed in the morning session and 24.1% in the afternoon session. More than a third (38.3%) of the subjects had a history of abdominal surgery. Fellows (under an attending physician’s supervision) performed 49.6% of the colonoscopies and the rest (50.4%) were performed by attending physicians. By indication, 71.2% of subjects underwent screening colonoscopy, 10.5% surveillance colonoscopy, and 18.3% diagnostic colonoscopy.

Demographic Characteristics of the Study Population
The variation of the mean TPT according to different factors is described in Table 2. Women, older individuals, and those with a past history of abdominal surgery had shorter TPTs (p-values were 0.68, 0.79, and 0.07, respectively). Colonoscopy done in the afternoon session also had a shorter TPT (p=0.004). Endoscopists with less experience had longer TPTs (p=0.68). Screening and surveillance colonoscopies had longer TPTs than diagnostic procedures (p=0.01 and p=0.008, respectively). Overall, the F value for the multiple regression model was 0.0009. The model predicts that TPT for colonoscopy (in minutes)=20.4+0.11(BMI)+2.41 (surveillance)+1.59 (screening)+0.33 (fellow)–2.11 (post meridiem)–0.01 (age)–0.2 (woman)–0.93 (abdominal surgery)±8.0.
Mean Total Procedure Time across Different Factors
DISCUSSION
Currently, there are a number of CRC screening strategies available, ranging from noninvasive tests such as the fecal occult blood test, fecal immunochemical test, fecal DNA test, and virtual computed tomographic colonography, to invasive sigmoidoscopy and colonoscopy tests. Among these, colonoscopy remains the most sensitive and is the gold-standard screening test. The demand for colonoscopy has risen in the past few years and is expected to rise further due to persistent efforts to spread awareness regarding CRC screening options among the general population. This puts pressure on the endoscopy suites to schedule the colonoscopy procedures in a time-sensitive manner to achieve maximum efficacy.
Based on our literature review, our study is the first of its kind. Our study examined various pre-procedure variables to accurately predict the procedure time required for each individual colonoscopy in order to help avoid inadvertent waiting times in the endoscopy suite. To better appreciate the true association, we excluded subjects with poor bowel preparation and those that required any intervention during colonoscopy to ensure our study results are free of bias.
Overall, our model had an F value of 0.0009, which is a statistically significant number. We found that women had, on average, shorter TPTs (p>0.05). There is mixed evidence in relation to sex and difficult colonoscopy. Women have a longer colon with a higher tendency to dip into the pelvis and a smaller abdominal cavity; thus, creating more looping, making it harder to navigate through the colon to reach the cecum [8]. Our population was predominantly composed of African-Americans and we attribute this unexpected finding about sex to the typical body habitus of African-Americans. In a recent study, cecum intubation time was found to be shorter for women in a population composed predominantly of African-Americans [9].
We also found that older individuals tended to have shorter TPTs (p>0.05). There is evidence to suggest that cecum intubation is more difficult in older versus younger subjects, although the older population tends to tolerate the procedure better [10]. The reason for the apparently contrary trend in our population is not clear.
General abdominal surgery leads to intraperitoneal adhesions in 67% to 93% of subjects [11,12]. Abdominal hysterectomy is a risk factor for prolonged cecum intubation during colonoscopy [13]. In our study, we found a negative but non-significant association between abdominal surgery and TPT, opposite of the expected trend. We included all subjects with a history of abdominal and pelvic (both open and laparoscopic) surgery as a high-risk category but excluded those with a history of hernia repairs. The incidence of abdominal adhesions post-surgery depends on the indication, approach, and nature of the surgery [14]. Lack of accurate data and non-inclusion of patients with hernia repair in the high-risk category is the most likely explanation for the lack of the expected trend.
Obese subjects were found to require longer time for the colonoscopy, consistent with our initial hypothesis. Very thin and obese subjects are both considered challenging to scope. This is because of increased looping and angulation in a lean subject or because of the difficulty in applying positional maneuvers in an obese subject during colonoscopy. The evidence is conflicting, but most believe that there is an optimal BMI for the so called “easy colonoscopy [5].” The study results suggest an increase in TPT by 0.11 minutes for an increase in BMI by a factor of 1.0. Although this trend is consistent with the current literature, in our study it did not reach statistical significance (p>0.05).
Operator’s experience is one of the key determinants of TPT. As expected, the procedure time for colonoscopy performed by a fellow was longer by 0.33 minutes when compared to one performed by an attending physician in our study results (p>0.05). Although the absolute difference is not large, the trend is suggestive of an association, which needs further exploration in future studies.
We used procedure indication as one of the possible pre-procedural factors expected to have an impact on the TPT. We hypothesized that the indication changes the endoscopist’s pre-test probability for finding a lesion/polyp and should affect the time spent in the inspection phase of colonoscopy. Interestingly, our study results do support an association between TPT and colonoscopy indication. Although we suspect that this trend is being driven by the inspection phase of colonoscopy we could not confirm it due to lack of individual withdrawal time data on our subjects.
Based on our study results, a surveillance or screening colonoscopy is expected to take, respectively, 2.41 and 1.59 minutes longer than a diagnostic colonoscopy. The association was statistically significant with a p=0.01. This association raises a few more interesting questions, such as whether the indication for a diagnostic procedure affects the TPT and also whether the minimum withdrawal time for a colonoscopy differs by indication. These questions need to be addressed with additional, well designed studies in future, which are also needed to confirm our study’s findings.
There is new evidence to suggest that colonoscopies done in the afternoon session tend to yield a lower adenoma detection rate due to increasing fatigue of endoscopists [5,15]. In addition, afternoon session colonoscopies tend to have poor bowel preparation quality due to the time lag between the bowel preparation agent and the planned procedure [5]. In our study, we found a statistically significant association between the timing of colonoscopy and the TPT. The procedures done in the afternoon took less time than those done in the morning. Because we excluded subjects with poor bowel prep and those requiring any intervention, the reason behind this trend is still open to debate. One plausible reason is that as the day progresses, the tired endoscopist unconsciously tries to finish each scheduled procedure in a shorter time span. This may mean that the minimum withdrawal time for a non-diagnostic colonoscopy should be longer for procedures done in the afternoon.
Based on multiple regression analysis of our study results (Table 3) and the identified associations, we can predict the TPT (in minutes) with the following equation=20.4+0.11 (BMI)+2.41 (surveillance)+1.59 (screening)+0.33 (fellow)–2.11 (afternoon)–0.01 (age)–0.2 (woman)–0.93 (abdominal surgery)±8.0.

Multivariate Regression Analysis
Our study being retrospective in design comes with unavoidable drawbacks of inaccurate data reporting. A few trends (e.g., the association between abdominal surgery and a shorter TPT) inconsistent with the current literature may be due to the lack of accurate data. Also, since ours is a single-center study with the majority of the participants being African-American, our results may not be generalizable.
Our study is the first to identify a way to predict TPT for each individual colonoscopy by considering known pre-procedural factors. Consequently, there is no exact literature to compare our results to, except for extrapolating results from other related studies. Our study has interesting results, some consistent with our a priori hypothesis and some contradicting current beliefs. Our study is well-designed in terms of inclusion and exclusion criteria, which reduced the risk of bias. The study is large enough to have sufficient power to achieve statistical significance (F value of 0.0009). It is expected that accurate prediction of colonoscopy TPT will help endoscopy suites increase their efficacy and patient satisfaction.
Our next step will be to validate our predictive model in a prospective study. Additional studies across different populations, with sub-analyses of time spent in the intubation and withdrawal phases of colonoscopy, are needed in future to accurately answer the questions raised by our study.
Notes
Conflicts of Interest: The authors have no financial conflicts of interest.