INTRODUCTION
Balloon tamponade is often used as a bridging therapy when immediate endoscopy or endoscopic control of variceal bleeding is difficult [1]. It is known to be particularly effective in treating massive variceal bleeding and is recommended by clinical guidelines [2]. SengstakenтBlakemore (SB) tube is the most widely used instrument for balloon tamponade [3]. Inflation of the esophageal and gastric balloon of the SB tube and anchoring it against the gastroesophageal junction are critical for adequate tamponade when using the SB tube. Appropriate SB tube placement results in successful hemostasis (40%т90%) [4]. However, it is associated with several major complications, including esophageal rupture, aspiration pneumonia, esophageal ulcers, and asphyxia resulting from balloon migration [3]. Impaction of the SB tube is a very rare complication, and endoscopic removal of an impacted SB tube has been reported in only 5 cases worldwide. In real clinical practice, impairment in liver function typically observed in patients requiring SB tube insertion is accompanied by hepatic encephalopathy. In grade 1 and 2 hepatic encephalopathy, the possibility of irritability in patients is increased, and the SB tube is transected and impacted. According to previous reports, most impacted SB tubes were deflated and easily removed endoscopically. However, under conditions when the SB tube is transected and the remnant tube remains inflated, endoscopic removal of the remnant tube is unknown endoscopically, and the choice of endoscopic tool is not established in this rare situation.
Here, we reported an exceedingly rare case of endoscopic removal of transected SB tube with inflated esophageal and gastric balloon.
CASE REPORT
A 53-year-old man with no history of specific disease presented with abdominal pain. He visited another hospital and underwent laboratory tests and abdominal computed tomography. He was diagnosed with chronic hepatitis B and liver cirrhosis (LC) associated with hepatocellular carcinoma (HCC) and was referred to our hospital for further work-up and suitable treatment.
At the time of admission, the patientтs blood pressure and pulse rate were 140/90 mm Hg and 90 beats per minute, respectively. Further, his breathing rate and body temperature were 22 breaths per minute and 36.4ТАC, respectively. Abdominal distension and shifting dullness were observed, whereas no palpable mass, tenderness, or rebound tenderness was detected in the abdomen. The results of complete blood cell count were as follows: white blood cell count, 5,630/mm3; hemoglobin, 9.7 g/dL; hematocrit, 28.5%; and blood platelet count, 73,000/mm3. Moreover, the results of serum biochemical test were as follows: total protein, 6.0 g/dL; albumin, 1.8 g/dL; total bilirubin, 1.53 mg/dL; aspartate aminotransferase, 95 IU/L; alanine aminotransferase, 15 IU/L; alkaline phosphatase, 697 IU/L; gamma-glutamyltranspeptidase, 166 IU/L; blood urea nitrogen, 19.4 mg/dL; and creatinine, 1.0 mg/dL. Prothrombin time and activated partial thromboplastin time were within normal limits.
Abdominal ultrasonography, dynamic magnetic resonance imaging, and esophagogastroduodenoscopy (EGD) were performed, and ultimately, the patient was diagnosed with LC, HCC infiltrating both the liver lobes with portal vein thrombosis, grade 2 esophageal varices with red color sign, and type 2 gastroesophageal varices (GOV2). On day 4 of hospitalization, he underwent prophylactic endoscopic variceal ligation (EVL) and transarterial chemoembolization in accordance with the Barcelona Clinic Liver Cancer guidelines for HCC. Despite appropriate management, the patientтs liver function gradually deteriorated, and esophageal variceal bleeding (EVB) and hepatic encephalopathy recurred during admission.
On day 12 of hospitalization, he presented with hematemesis (400 mL of blood) resulting from EVB and was immediately transferred to the intensive care unit. EGD and therapeutic EVL, along with aggressive blood volume resuscitation and intravenous administration of terlipressin, were performed to control EVB but failed because of unstable vital signs and massive bleeding. SB tube insertion (All Silicone SengstakenтBlakemore TubeТЎ; Create Medic Co., Yokohama, Japan) was performed as subsequent treatment, and medical therapy including administration of terlipressin was continued. On day 13 of hospitalization, grade 2 hepatic encephalopathy developed, and the SB tube was abruptly cut off because of the patientтs irritability.
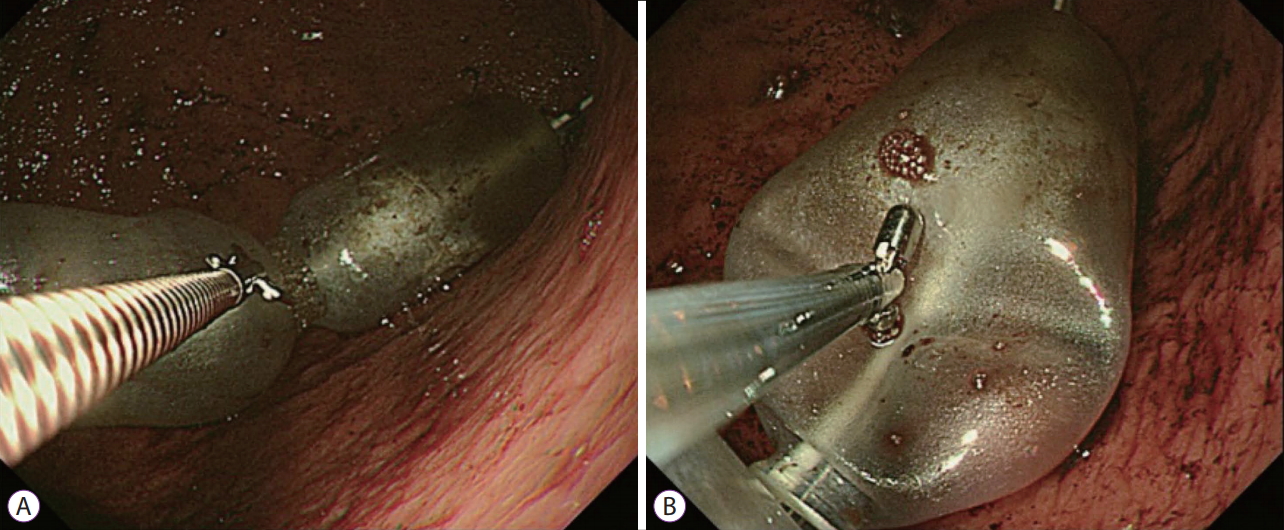
Emergency EGD showed esophageal and gastric balloon transection from the SB tube, which remained fully inflated and impacted. We attempted to deflate the balloon using various methods based on previous reports. Endoscopic injection needle (WS-2416PN2504; Omnimed Ltd., England, UK) and endoscopic cutter (FS-5L-1; Olympus, Tokyo, Japan) were initially used, but the balloon, having thick elastic walls, was not easily punctured. We subsequently used endoscopic hot biopsy forceps (FD-1U-1; Olympus) and employed argon plasma coagulation, which proved unsuccessful as the balloon, which was made of silicone, had excellent electrical insulating and heat-resistant properties. On the presumption that a sharper and more rigid instrument could cut the balloon, we finally chose and used endoscopic scissors (FS-3L-1; Olympus) to perforate the balloon (Fig. 1), and the deflated balloon was gently removed using an endoscopic snare (SD-210U-10; Olympus) without any complication (Fig. 2).
Discussion
EVB is a lethal complication of portal hypertension in patients with LC [5], with a mortality rate ranging from 12% to 20% during the acute episode, which, by consensus, refers to the first 5 days after patientтs hospital visit [3]. Over the past few decades, numerous treatment options for the management of EVB have been used, such as pharmacological vasoconstriction, physical compression via balloon tamponade, and diverse endoscopic interventions [5]. The recommended treatment for acute EVB is based on early and circumspect blood volume resuscitation and early administration of intravenous vasoactive drugs (terlipressin, somatostatin, or analogs) and prophylactic antibiotics. Within the first 6 to 12 h of admission following hemodynamic stabilization, EGD was used to confirm the origin of bleeding and perform endoscopic therapy [3]. EVL is the preferred endoscopic therapy for EVB, whereas endoscopic variceal obturation is recommended for acute bleeding resulting from GOV2 and isolated gastric varices [6]. The optimal endoscopic therapy for type 1 gastroesophageal varices remains controversial [7].
However, the recommended treatment fails to control bleeding in 10%т20% of cases [8]. If standard therapy fails to control EVB or patients are hemodynamically unstable to undergo endoscopic procedure, balloon tamponade using an SB tube is the next treatment option [1,2]. Although other endoscopic procedures such as self-expanding metal stenting can be employed, SB tube insertion remains to have a role to play in the management of EVB [2]. Nevertheless, SB tube insertion is accompanied by various complications, some of which are major or minor events [9]. In our case, definitive airway protection was provided before SB tube placement to prevent various complications. The gastric balloon was placed in the stomach fundus and inflated with 250 mL of air, whereas the esophageal balloon was inflated to a pressure of 30 mm Hg and deflated every 6 h.
Among various complications, impaction of the SB tube is exceptionally rare, and endoscopic removal of the impacted SB tube has been reported in only 5 cases worldwide (Table 1). In 1985, Gossat and Bolin [10] reported a case of endoscopic removal of inflated esophageal and gastric balloon transected from the SB tube using endoscopic biopsy forceps. In contrast, Chawla et al. [11] in 1988 and Kim et al. [12] in 2006 reported a case of endoscopic removal of inflated gastric balloon not transected from the SB tube using endoscopic sclerotherapy needle and using endoscopic needle knife and sclerotherapy needle, respectively, whereas Ko et al. [4] in 2010 reported a case of endoscopic removal of inflated gastric balloon transected from the SB tube using endoscopic injection needle. Moreover, in 2013, GonУЇalves et al. [13] described a case of endoscopic removal of deflated esophageal and gastric balloon transected from the SB tube using endoscopic snare. As in previously reported cases, forcefully pulling the inflated balloon of the SB tube must be avoided to prevent lethal complications such as hemorrhage, perforation, and airway obstruction [4,12].
SB tube was transected in our case, unlike in the cases reported by Ko et al. [4] and GonУЇalves et al. [13], because of the patientтs irritable movement rather than SB tube deformation resulting from inappropriate sterilization and reuse or from manufacturing defect. Being a new product, the SB tube was carefully inspected prior to intubation. To prevent various complications associated with SB tube insertion, it is important not only to fully understand the procedure and inspect the SB tube before insertion but also to closely monitor the patient after intubation [4].
We attempted to puncture the inflated gastric and esophageal balloon transected from the SB tube using endoscopic injection needle, as reported by Ko et al. [4], and endoscopic hot biopsy forceps and argon plasma coagulation, similar to Kim et al. [12], but to no avail. In our case, because of the excellent electrical insulating and heat-resistant properties of the SB tube, which was made of silicone, the use of endoscopic hot biopsy forceps and argon plasma coagulation might not have worked. Various factors including endoscopistsт technique, sort of instrument such as endoscopic injection needle type, and balloon characteristics may have an effect on the success of balloon puncture. In our case, we presumed that a sharper and more rigid instrument might work and finally used endoscopic scissors to puncture the balloonтs thick and elastic walls.
To the best of our knowledge, no previous report has described the endoscopic removal of impacted esophageal and gastric balloon transected from the SB tube, which is extremely rare, using endoscopic scissors. Here, we reported a very rare case of endoscopic removal of inflated transected SB tube using endoscopic scissors. After intubation, close patient monitoring is crucial, and appropriate sedation can be used to prevent SB tube transection owing to the patientтs irritable movement [4]. If the SB tube is transected and its esophageal and gastric balloon remains inflated, leading to impaction, endoscopic removal using endoscopic scissors can be considered an effective treatment option.