INTRODUCTION
It is difficult to differentiate early-stage gastrointestinal cancers from inflamed mucosa using white light imaging (WLI) alone despite the high resolution of endoscopic images. Image-enhanced endoscopy has progressed since the early 2000s and includes narrow band imaging (NBI), flexible spectral imaging color enhancement (FICE), and i-Scan. The usefulness of these endoscopic methods in the diagnosis of gastrointestinal lesions with/without magnification has been discussed. FICE yields bright and high-contrast images of gastrointestinal lesions [1,2]. However, the imaging of irregular microvessels in malignant lesions is insufficient at high magnification. NBI is excellent in demonstrating the irregular microvessels of gastrointestinal cancers at high magnification [3-5]. This technique does have limitations, producing dark images of distant lesions in a large luminal organ such as the stomach and poor visualization of mucosal microstructure on the tumor surface [6], which is not appropriate for screening endoscopy. The advent of new endoscopic systems is expected to resolve these problems. Recently, multilight imaging technology using linked color imaging (LCI) and blue laser (light) imaging (BLI) systems (Fujifilm Co., Tokyo, Japan) has been developed to resolve the limitations of existing image-enhanced endoscopic modalities. The push of a single button during endoscopy allows one to switch between LCI and BLI. In addition, they facilitate both screening and detailed observations of the gastrointestinal tract because of a longer observable distance than that provided by NBI. LCI and BLI use a simpler procedure than NBI, enabling widespread use of this system [6]. These new endoscopic imaging modalities facilitate new diagnostic approaches in gastrointestinal lesions [7,8].
In this review, we carried out a search of the PubMed database for studies published until July 2018 using the keywords ŌĆ£LCI, linked color imaging, BLI, blue laser imaging, Helicobacter pylori eradicationŌĆØ and identified relevant literature for this review. The references cited in these papers were also checked to complement the search. LCI and BLI are the latest imaging modalities but have only been reported sporadically in the English language literature for their usefulness in identifying upper gastrointestinal lesions, despite an extensive search of existing literature. This review was undertaken to describe the potential applications of LCI and BLI. We review LCI and BLI as well as the present and future status of these imaging modalities and describe their usefulness in clinical practice.
INTRODUCTION TO LCI AND BLI
Wavelength and color information in endoscopic systems
The characteristics of LCI, BLI, and WLI are shown in Table 1. The emission intensity at short wavelengths in LCI and BLI is much higher than that in WLI. LCI and BLI clearly depict the mucosal surface including the microstructure because of the high intensity at short wavelengths including 410 nm (blue violet) and 450 nm (blue). Particularly, 410 nm wavelength reflects microstructure and microvasculature in the superficial layer of the mucosa. LCI is obtained from BLI-bright by computerized image processing. Therefore, the emission intensities (in descending order) at this wavelength are the highest with BLI, followed by BLI-bright (LCI) and WLI. Differences in emission intensity largely influence the color and structure seen in mucosal surface images. BLI, with the highest intensity, visualizes the surface pattern with the greatest detail.
BLI and BLI-bright have blue and green color information, while LCI has additional red information. LCI shows mucosal color similar to WLI but interestingly produces more color patterns of the mucosa due to emission intensity at wavelengths different from WLI. The brightness (in descending order) of these modalities is greatest in LCI, followed by WLI, BLI-bright, and BLI. LCI is the brightest and thus most useful when screening for gastrointestinal lesions even at a distant view in a wide-lumen organ such as the stomach.
Color recognition of upper gastrointestinal lesions for screening
LCI and BLI produce several color images and yield detailed information about structure and vessels, neither of which is achieved with ease when using WLI. LCI expands small differences in colors, making them easy to recognize, which may be due to differences in reflectance at short wavelengths from the superficial layer of the mucosa. The reflectance at short wavelengths is different among tissues with various histological changes in the gastrointestinal mucosa [9]. For example, the color of malignant gastric lesions is similar to that of the surrounding mucosa using WLI, but their reflectance at short wavelengths is extremely different. Both LCI and BLI have high emission intensity at short wavelengths, especially 410 nm [7,8], and thus highlight differences in spectral reflectance among tissues with various histological changes in the images produced, leading to high color contrast between those areas resulting in easier recognition of lesions (Table 1).
Selecting LCI or BLI for screening
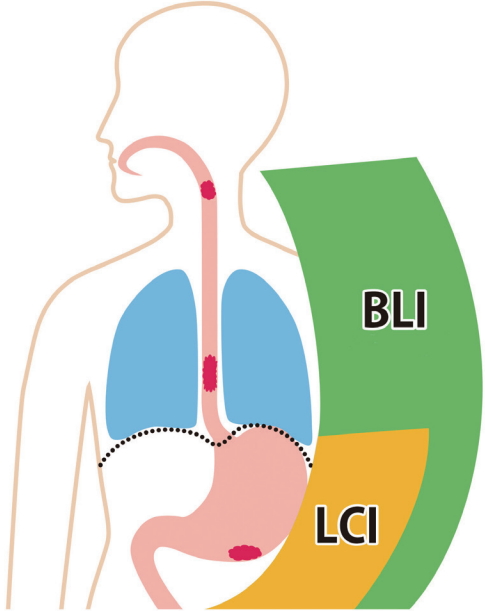
Laser and LED endoscopy are important for screening and performing detailed examinations of upper gastrointestinal lesions. Image-enhanced endoscopy has not been commonly used for screening, and most endoscopists have little experience using it despite the benefits for patients. One must first decide whether to use LCI or BLI (BLI-bright) to identify lesions when screening. No data have been reported showing a comparison of images from LCI and BLI, but it is essential to detect cancers more effectively in a short time during endoscopy when screening. If one mode is more effective in screening for esophageal cancers than another mode, it is not necessary to discuss their effectiveness, comparing images from the two modes. Based on our extensive clinical experience to date with upper gastrointestinal lesions, we summarize the use of these modes in Fig. 1.
Detecting early gastric cancers through screening may allow endoscopic resection, thus obviating the need for surgical resection, resulting in improved patient quality of life [10]. LCI is brighter than WLI, and BLI is brighter than NBI [7,8]. LCI produces particularly bright images in a wide-lumen organ such as the stomach and are useful when screening for gastric lesions, whereas BLI-bright and BLI are also useful in displaying mucosal structure and vessels in close-up views inside the stomach. However, endoscopists should be aware that relatively close views using BLI allows screening even in the stomach, especially the antrum, because the images are brighter than that in NBI.
In contrast, the larynx, pharynx, and esophagus all have narrow lumens with squamous cell epithelium [11]. Endoscopic findings for these epithelia are characterized by microvessels on the mucosal surface rather than microstructure. Intrapapillary capillary loops in the superficial mucosa are important in the diagnosis of neoplastic lesions. BLI has higher emission intensity at short wavelengths and is more suitable in the diagnosis of intrapapillary capillary loops in such areas than LCI.
The importance of color to establish a diagnosis
Some characteristic colors of upper gastrointestinal lesions observed on LCI and BLI are shown in Table 1. The apparent color of lesions using these modes can be determined not only with one color but also by mixing two colors in the respective gastrointestinal organ. The advent of bright image-enhanced endoscopy with modalities such as LCI and BLI requires the endoscopist to carefully observe and recognize mucosal colors during screening endoscopy. These colors allow endoscopists to diagnose a variety of lesions, including malignancies, and areas of inflammation because of the high color contrast with surrounding mucosa.
ESOPHAGUS
Superiority of BLI in detecting squamous cell carcinoma
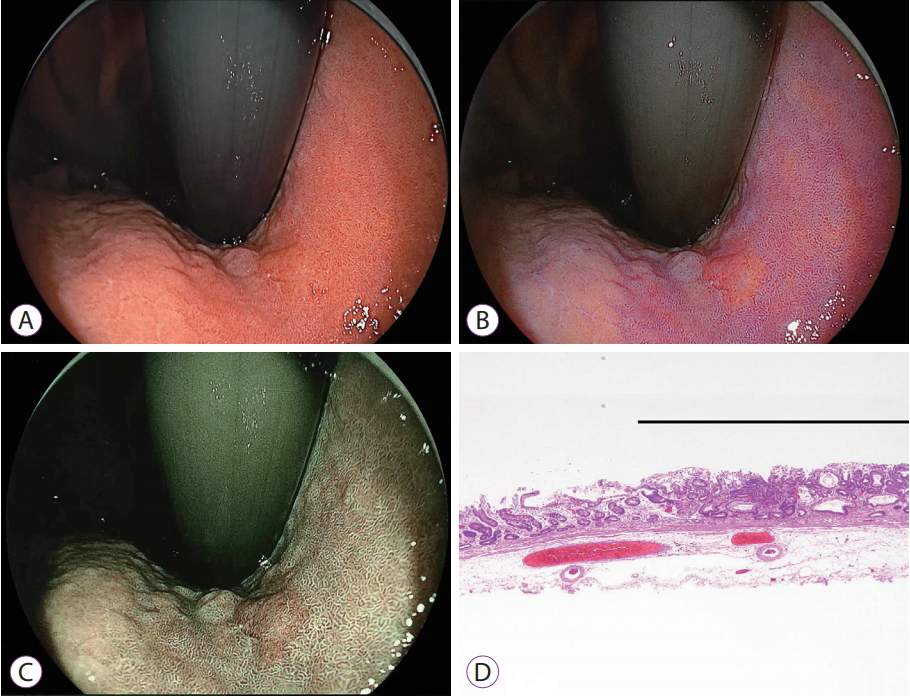
In squamous cell carcinomas of the esophagus, BLI reveals a higher color contrast between brown lesions with intrapapillary capillary loops and the surrounding area in detail [15]. BLI has been used for early recognition of esophageal cancers in screening programs [8,16,17]. BLI images may seem similar to images obtained by NBI; however, there is a great difference in the composition of wavelengths of these two modalities. An NBI image consists of spectral images alone, whereas BLI images are created from both spectral and white light images. The difference in these characteristics may influence brightness, far-field of view [6], depth of focus, and demonstration of microvessels in the esophageal mucosa. BLI is reported to be useful in the recognition of early esophageal cancers as brownish areas and dot-forming vessels without magnification [8]. In addition, the ranking score for detection and mean color difference score of BLI-bright were significantly higher than that of WLI and NBI [17]. Images of early cancer in the mid-portion of the esophagus are compared using WLI, LCI, and BLI in Fig. 2. WLI does not show abnormal features suspicious of malignancy. However, BLI can enable visualization of a brown malignant lesion distinct from the surrounding mucosa, but LCI cannot. Although experience using image-enhanced endoscopy is not yet based on rigorous data, BLI can detect early brown esophageal cancers, but LCI cannot in some cases, suggesting that BLI may be superior to LCI and WLI. Most esophageal cancers have a similar color pattern in BLI during screening. Some endoscopists may prefer to use BLI-bright, which display images of more distant mucosa as well [17]. BLI (BLI-bright) use is strongly recommended in screening for early esophageal cancers with transoral endoscopy and even with transnasal endoscopy. Endoscopists should keep in mind that some early esophageal cancers cannot be detected using LCI or WLI.
Findings in BarrettŌĆÖs esophagus and adenocarcinoma
Existing image-enhanced endoscopy modalities are useful in the diagnosis of BarrettŌĆÖs esophagus [18]. LCI also improves the visibility of short-segment BarrettŌĆÖs esophagus compared with WLI, especially for trainees, when evaluated both subjectively and objectively [19]. The extent of BarrettŌĆÖs esophagus is easily shown on images with high color contrast with the gastric mucosa using LCI and BLI. In addition, BLI facilitates the early detection of synchronous adenocarcinomas in patients with BarrettŌĆÖs esophagus [16], although data in LCI has not yet been reported.
STOMACH
Early gastric cancer with chronic H. pylori infection
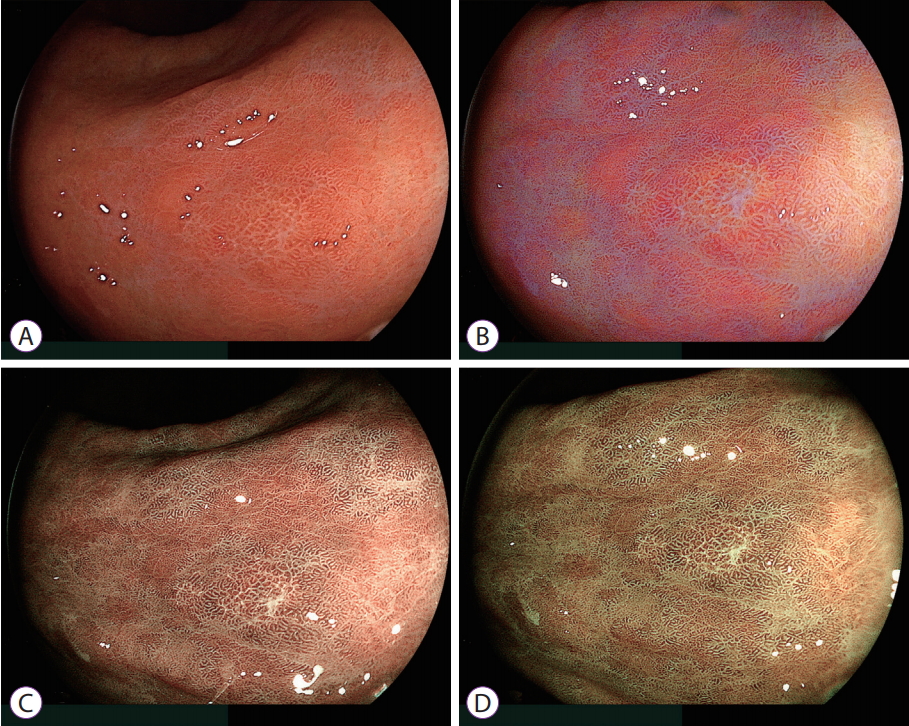
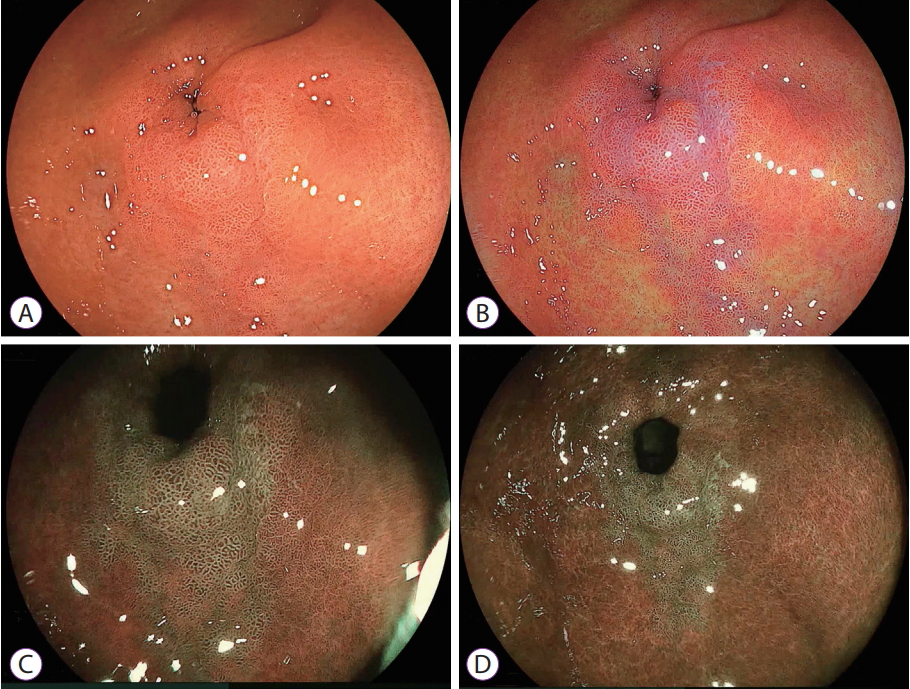
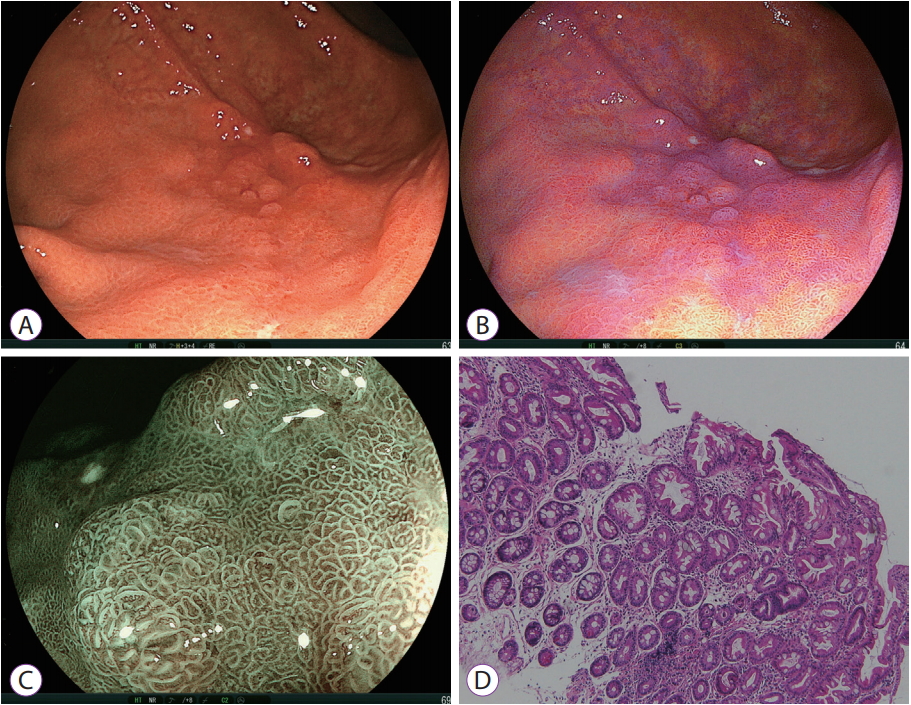
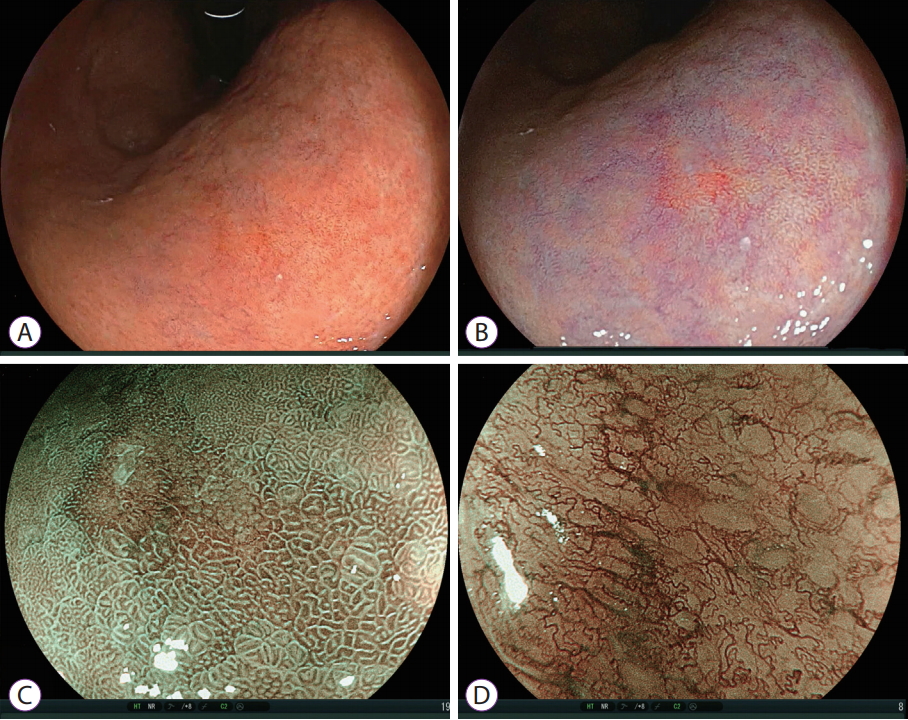
Most gastric cancers occur in the background of chronically inflamed mucosa due to H. pylori infection. The early detection of gastric cancer is difficult in such background mucosa, even for well-trained endoscopists, and early gastric cancers are frequently missed in WLI [20]. Precise diagnosis and growth of these lesions have been well studied because of the development of magnifying and image-enhanced endoscopy. However, the usefulness of image-enhanced endoscopy in the early detection of gastric cancer in the distant view remains unknown to many endoscopists. LCI shows a difference in color between a malignant lesion and the surrounding mucosa, allowing enhanced recognition of early gastric cancers without magnification (Figs. 3-6) [13,14]. Most early gastric cancers are seen as orange-red, orange or orange-white in LCI. Orange-red or orange areas changed from the color similar to the surrounding mucosa in WLI. Orange-white areas changed from discolored mucosa in WLI. The colors of gastric cancer in LCI produce high color contrast with the surrounding purple mucosa.
A few cancers with a more intense red color appear to be purple. These color patterns are important for the early detection of gastric cancers. LCI can detect multiple flat cancers that had been missed by WLI alone [13]. Flat cancers may be surrounded by purple mucosa with high color contrast. Color patterns are useful for metachronous gastric cancers that have been reported following curative endoscopic resection of early gastric cancer [21]. In addition, it is surprising to detect even quintuple small early gastric cancers using LCI.
Detecting early gastric cancers in areas of intestinal metaplasia
Most gastric cancers develop in areas of background chronic gastritis, especially with intestinal metaplasia (Figs. 3-6). Ash-colored nodular changes are an endoscopic sign of gastric intestinal metaplasia using WLI. However, the sensitivity of endoscopic diagnosis of intestinal metaplasia using WLI is lower compared to the sensitivity of histopathological diagnosis [22]. It is difficult to diagnose gastric intestinal metaplasia in areas of chronic gastritis despite the high risk for gastric cancer [7,22-24]. Preliminary data from LCI and BLI show that gastric intestinal metaplasia can be seen as a purple and green mucosa with a patchy distribution on screening examinations, respectively [7,8,25]. These modalities help to identify gastric intestinal metaplasia that occurs in a focal area (Fig. 7) and spreads over a broad area (Fig. 3).
LCI images metaplasia as deep or pale purple mucosa even in the distant view. Endoscopists should be aware that strong color (tone) enhancement (C2ŌĆōC3) by the processor can produce a deep purple color in areas of gastric intestinal metaplasia, which is recognized with ease. If endoscopists cannot judge whether the mucosal color is pale purple or another color, changing to BLI allows for the recognition of green mucosa, strongly suggestive of intestinal metaplasia [7,8].
Purple and green mucosal areas seen in LCI and BLI are important for the following two reasons, respectively: (1) Early gastric cancer can be detected in a background of intestinal metaplasia with high color contrast. (2) Gastric intestinal metaplasia can be diagnosed in a depressed area with morphological features similar to gastric cancer, ruling out malignancy.
Malignant lesions are surrounded by intestinal metaplasia in most endoscopically resected specimens [7,12-14]. These types of mucosae have been reported to lie adjacent to each other in surgically resected specimens [26-28]. Therefore, a finding of purple mucosa is likely to correspond histologically to intestinal metaplasia. These features may facilitate recognition of early gastric cancers during screening examinations.
Purple mucosae are consistent with areas of green mucosa demonstrated by BLI. BLI can also produce high color contrast between malignant gastric lesions and the surrounding mucosa (Figs. 3-6) [7,8] and is useful in screening for gastric cancers especially in the antrum (Figs. 3, 4). Endoscopists should notice that the volume of the antrum is smaller than that of the gastric body. At close-up and in magnified views, BLI can produce high color contrast between a malignant lesion and the surrounding mucosa and exhibit microstructural and microvascular patterns in detail [7,8]. The degree of color contrast is remarkably different between C1 and C2 using the image processor color (tone) enhancement function (Fig. 4). C2 color enhancement results in strong green enhancement, which appears as deep green mucosa, especially in areas of gastric intestinal metaplasia. In addition, deep green intestinal metaplasia shows a patchy and flat-sheet pattern of distribution in the background mucosa and surrounds gastric cancers (Figs. 3-6) [7,8]. The apparent line of demarcation between a brown malignant lesion and the surrounding green mucosa allows endoscopists to recognize cancers and mark the site precisely before performing endoscopic submucosal dissection (ESD) for complete resection. Purple and green gastric intestinal metaplasias play an important role in the recognition of early gastric cancers using LCI and BLI, respectively.
It is also important for endoscopists to rule out malignancy and definitively diagnose the inflammatory mucosa. Endoscopists must consider what precedes the establishment of a diagnosis of a gastric lesion-changes in color or morphology. On screening endoscopy, a diagnosis of a gastric lesion is established based, mainly, on the distinctive morphology of a lesion with respect to the surrounding mucosa. However, this method sometimes leads to a misdiagnosis. The spectral reflectance of a malignant lesion differs from that of a benign lesion [9], based on a physiological mechanism that cause a difference in mucosal color. In a recent report, LCI was shown to provide more information to endoscopists, and allows for the differential diagnosis of a lesion based on mucosal color [13,14,29]. This characteristic suggests that LCI may rule out a malignancy based on color even for a morphologically abnormal lesion that looks like a malignancy imaged with WLI. For example, with the image shown in Fig. 8, most endoscopists would diagnose the depressed lesion as suggestive of gastric cancer or mucosa-associated lymphoid tissue lymphoma using WLI. However, LCI shows a relatively homogenous purple mucosa in the entire depressed area, suggesting gastric intestinal metaplasia. All three biopsy specimens revealed intestinal metaplasia. Endoscopists should be aware that the alterations in the mucosal color of lesions precedes changes in morphology in LCI, which may be a new approach to differentiate lesions with abnormal morphology.
Early gastric cancer after H. pylori eradication
Successful H. pylori eradication brings dramatic changes in inflammation and acid-related molecules in the gastric mucosa [22,30,31]. Prophylactic eradication of H. pylori after endoscopic resection of early gastric cancer should be performed to prevent the development of metachronous gastric carcinoma [32]. However, gastric cancers may be found in patients who were treated for H. pylori eradication [33,34], and endoscopists may have difficulty in establishing the diagnosis endoscopically. Surprisingly, early gastric cancers may have a surface pattern similar to the pattern of changes noticed with chronic gastritis. This results from a gastritis-like appearance, due to the non-neoplastic epithelium covering the malignant tissue, resulting in an indistinct border or lack of obviously malignant characteristics [35,36]. NBI magnifying endoscopy can demonstrate pattern differences relative to the surrounding non-malignant mucosa, and it is important to detect this difference [36]. However, these findings make it difficult for many endoscopists to diagnose such lesions even with NBI magnifying endoscopy. Endoscopists need a new diagnostic method to make it easier to detect such malignancies.
LCI and BLI have not been discussed in relation to gastric cancer after successful H. pylori eradication. However, early gastric cancers are encountered after successful eradication and have been precisely diagnosed as cancer with an apparent demarcation line using LCI and BLI. Interestingly, the color contrast between early gastric cancers and the surrounding mucosa in H. pylori-eradicated mucosa is similar to what is observed in H. pylori-infected mucosa. In Fig. 6, slightly pale mucosa can be seen along the greater curvature at the gastric angle on WLI. LCI shows orange-red mucosa surrounded by purple mucosa at a distant view. BLI also shows brown mucosa surrounded by green mucosa at a close view. The exact line of demarcation can be determined by examining both images with high color contrast. However, the close-up and magnified views obtained using BLI reveals gastritis-like features on the mucosal surface, with a brown malignant area, similar to that of the surrounding green mucosa. Therefore, the surface pattern features make it difficult to differentiate malignant lesions from changes due to chronic gastritis. Endoscopists should pay attention to the color images obtained by LCI and BLI without magnification, both of which clearly show a difference in the color of the mucosa in malignant and surrounding areas. It is important to understand that color findings may precede morphological findings of malignant lesions when diagnosing them in H. pylori-eradicated mucosa.
Detecting early gastric cancers among erosions or multiple tiny gastric lesions
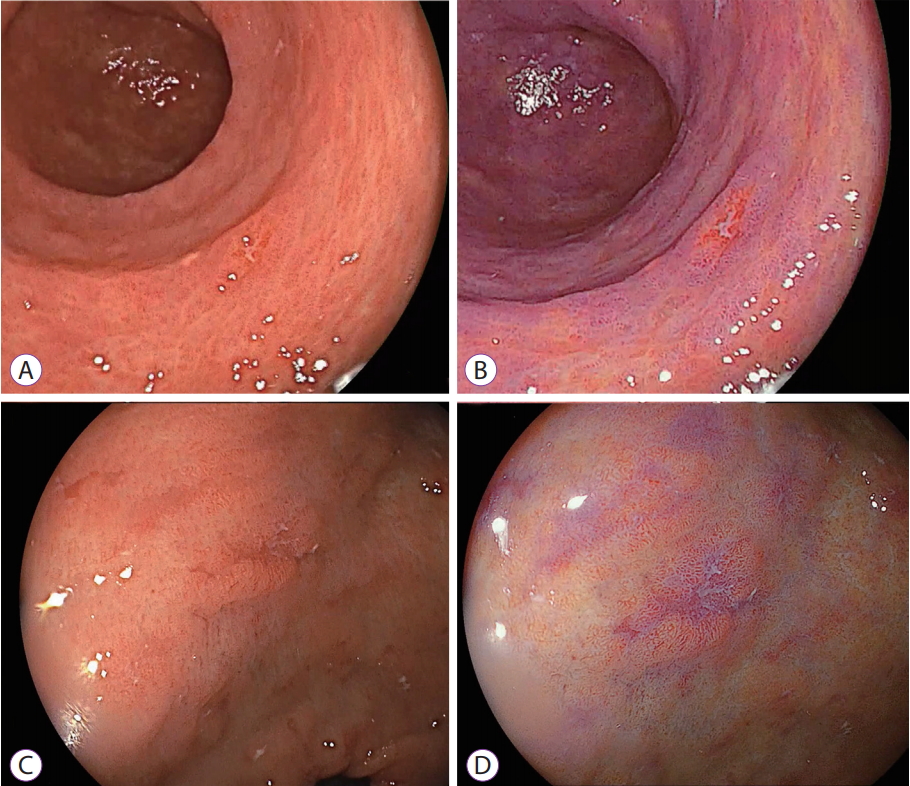
Gastric lesions appear in various forms and colors in acute and chronically inflamed mucosae. These lesions may appear as mucosal roughness, erosions, plaques, abnormal colors, bumps, or pitting when observed by conventional endoscopy. Image-enhanced endoscopy with magnification may be useful in differentiating such inflamed mucosae from early gastric cancer and precancerous lesions [37]. LCI and BLI have the advantage of showing distinctive findings, making it possible to differentiate these lesions without magnification. The effectiveness of LCI in areas of erosive inflamed mucosa has not been reported. Small regenerative changes in gastric erosions and small gastric cancers have a similar color and morphology when imaged with WLI, and biopsy is often necessary to differentiate them with precision. Endoscopists may not be able to recognize the difference in these lesions using WLI because they are too small to differentiate definitively. However, even such small lesions can be recognized using LCI based on their difference in color. In Fig. 9, two small lesions (Fig. 9A, C) seem to be erosive inflamed mucosae when imaged with WLI. Malignant lesions are characterized by an orange-reddish depressed form (Fig. 9B) and erosive inflamed mucosae by a purple depressed form (Fig. 9D). LCI may be useful in detecting cancer among such small lesions, but a prospective study is warranted to evaluate this conclusively.
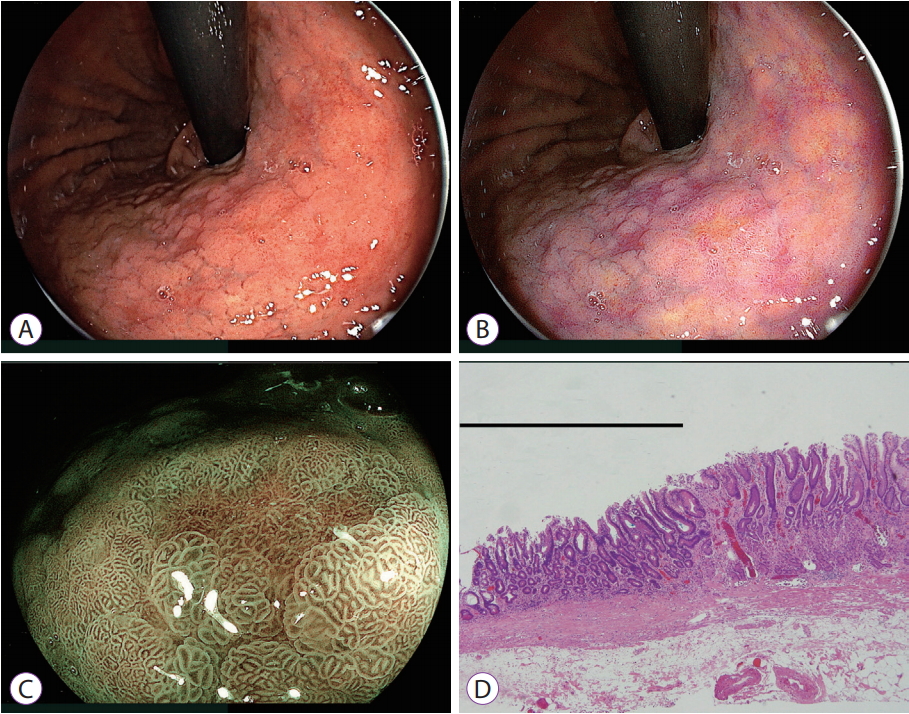
It is difficult to detect cancer among multiple depressed lesions of the stomach, which are often encountered in areas of chronic gastritis on screening endoscopy, using WLI alone. A malignant lesion may be hidden in such areas, but until recently, no endoscopic method for detection was available. Chronic gastritis appears in several color patterns in LCI and BLI [7,12-14]. However, LCI has the potential to detect malignant lesion among such lesions, distinct from inflammatory changes. In Fig. 10, at a distant view, the malignant lesion is recognized as orange mucosa, distinct from multiple inflammatory depressed areas of the mucosa, which appear as purple mucosa. Orange-colored lesions could be identified as early gastric cancers, supported by BLI magnification. The ESD specimen shows well-differentiated adenocarcinoma. On screening, endoscopists should be mindful of the different colors among irregularly shaped areas of the gastric mucosa when using LCI rather than WLI.
Early gastric cancer without H. pylori infection
No data is available regarding the detection of early gastric cancers using LCI and BLI in normal background mucosa that is not infected with H. pylori. However, we have observed the effectiveness of LCI in some patients in the clinical practice. Endoscopists must know whether the color of a cancer is similar to the color of a H. pylori-infected background mucosa. In Fig. 11, an elevated lesion similar to that observed with erosive changes is seen near the pyloric ring in WLI. BLI magnification shows a relatively regular surface pattern in the central portion. However, LCI demonstrates an orange lesion on the surface mucosa, suggesting a malignant lesion. Pathological evaluation of the resected specimen shows a well-differentiated adenocarcinoma.
Undifferentiated gastric cancer
Magnified BLI reveals irregular and distinctive microvessels, which are present in undifferentiated gastric carcinoma [7,8]. A key fret pattern or ŌĆ£frizzyŌĆØ vessel is a characteristic feature in an unstructured area [7]. High-resolution images in good focus are greatly useful in diagnosing uneven malignant areas in BLI [8], but no data have been reported regarding the detection of undifferentiated cancers during screening. Endoscopists need to evaluate the images of undifferentiated gastric cancer using LCI without magnification. In Fig. 12, it is difficult to identify malignant lesions using WLI alone. LCI reveals a small orange-reddish lesion on the lesser curvature similar to that observed with a differentiated carcinoma. The surface pattern of most areas seems to be normal. The earliest undifferentiated carcinoma may have a normal surface pattern when viewed without magnification. Magnifying BLI in a slightly depressed area shows irregular microvessels in an unstructured area suspicious for undifferentiated carcinoma. LCI has the potential to detect undifferentiated gastric carcinomas based on their color in the mucosa seen as a suspicious malignant lesion although histology cannot be determined from endoscopic findings without magnification.
Transnasal endoscopy with LCI in detecting early gastric cancer
Small-caliber endoscopy has progressed with improved technology to deliver high-resolution images and is commonly used in Japan to screen for upper gastrointestinal lesions. LCI and BLI have been available with one small-caliber endoscope (e.g., EG-L580NW; Fujifilm Co.) using a laser endoscopic system since 2014 and with one (e.g., EG-740N; Fujifilm Co.) using an LED endoscopy system since 2018. These endoscopes are characterized by a small radius at the tip, which allows observation of upper gastrointestinal lesions with a frontal view [38,39]. A recent report showed that WLI using small-caliber endoscopy did not allow the diagnosis of a small red lesion as cancer, but BLI showed a discolored area around the red lesion with irregular vessels, resulting in the accurate diagnosis of an early case of gastric cancer [39]. Further studies of small-caliber endoscopy are warranted in the future.
DUODENUM
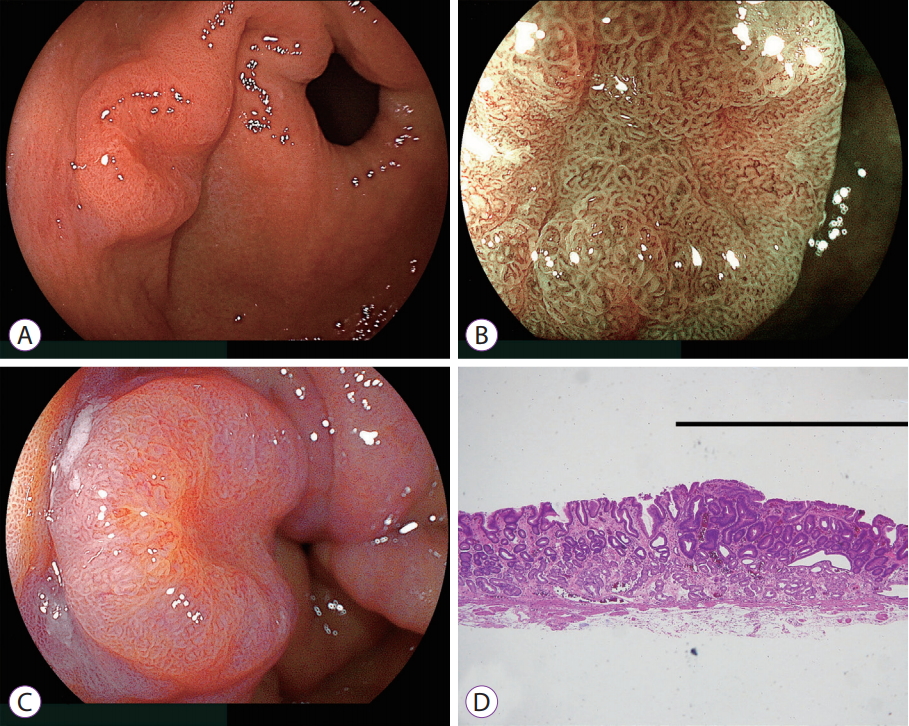
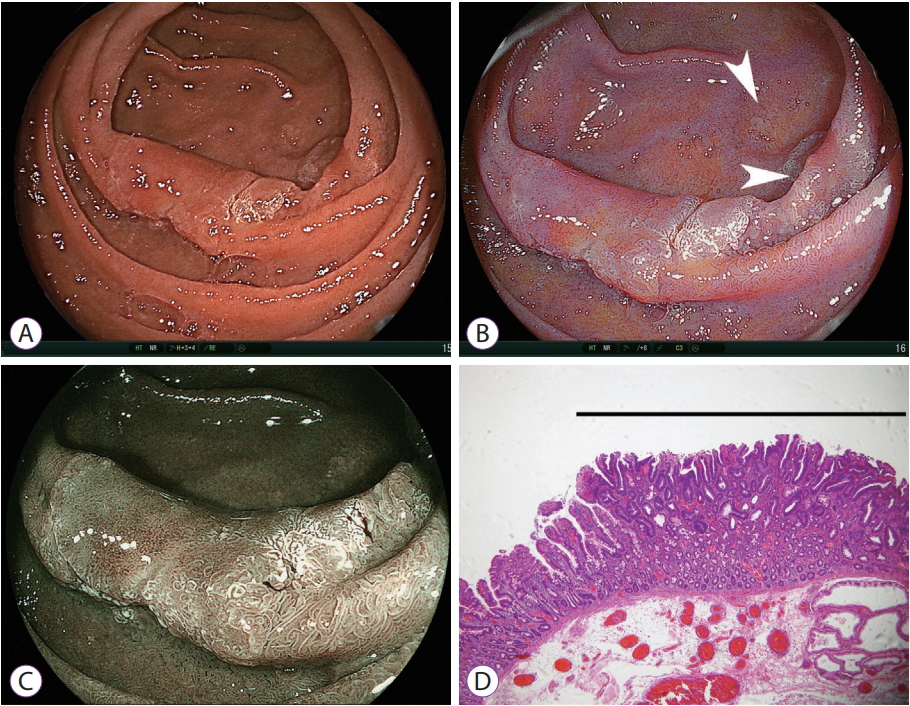
Colonoscopic resection of adenomatous polyps reduces the mortality from colorectal cancer because of the adenoma-carcinoma sequence [40,41]. The efficacy of removing sporadic duodenal adenomas is unknown. Duodenal neoplasms are the second leading cause of death in patients with familial adenomatous polyposis [42], and therefore, the resection of sporadic duodenal adenomas may be recommended. The use of endoscopic treatment for duodenal neoplasms has been increasing in Japan. ESD has been attempted for complete resection [43,44]. However, this technique is difficult, and recent reports recommend the use of simple and safe endoscopic methods, including underwater resection and cold snare polypectomy [45,46]. Therefore, endoscopists need accurate diagnoses before using these treatments. BLI detects not only vascular and surface patterns of duodenal cancer with magnification, but also the minute white opaque substance of possible fatty deposits on the tumor surface [8]. However, no data have been reported for LCI. Images of duodenal cancer are shown in Fig. 13. LCI shows an orange image in the area where histopathological findings reveal cancer in an adenoma and enhances the white opaque substance in the peripheral areas of the lesion, suggesting only an adenoma. However, some duodenal adenomas may appear to be orange in color. Further studies to characterize the imaging of duodenal neoplasms are necessary.
CONCLUSIONS
LCI may allow for a new endoscopic approach to screening, based on the premise that color changes precede morphological changes in the mucosa during visualization of gastric lesions. LCI can detect early gastric cancer in high color contrast with respect to the surrounding mucosa, irrespective of H. pylori status, and helps in the diagnosis of inflamed mucosa including erosions, distinct from cancers, based on color. LCI also shows duodenal cancers as orange-colored. BLI is superior to LCI in the detection of early esophageal cancer and provides microstructural and microvascular images at near and in magnified views. It is important to obtain both types of images alternately to establish a diagnosis.