INTRODUCTION
Intramucosal colorectal cancers without lymph node metastasis are good indications for endoscopic treatment [1-3]. Lymph node metastasis can be truly determined only by histopathologic examination of the surgical specimen, whereas endoscopic assessment allows only estimating the risk of invasion and metastasis [4]. Unfavorable histologic findings including submucosal invasion 1,000 ╬╝m, positive lymphovascular invasion, poorly differentiated adenocarcinoma, signet-ring cell carcinoma, mucinous carcinoma, or grade 2/3 budding at the site of the deepest invasion are considered risk factors of lymph node metastasis, requiring radical dissection or systemic treatment [5,6]. Therefore, estimation of the invasion depth is one of the most important steps in establishing the treatment strategies for colorectal cancer.
INDICATIONS FOR COLORECTAL ENDOSCOPIC SUBMUCOSAL
Colorectal endoscopic submucosal dissection (ESD) can achieve en bloc resection in >80% of the indicated cases [7]. However, it is still a technically challenging, time-consuming, and resource-consuming procedure, in addition to its high risk of adverse events.
The current indications for colorectal ESD vary among different countries. The Korean Heath Insurance Review and Assessment Service announced that the costs of colorectal ESD can be reimbursed for a well-differentiated mucosal cancer Ōēż5 cm without ulceration, a laterally spreading tumor (LST) Ōēź2 cm, a sessile polyp Ōēź2 cm, and an adenoma with fibrosis. The Japanese Colorectal ESD Standardization Implementation Working Group proposed that colorectal ESD should be indicated in lesions for which en bloc resection with snare endoscopic mucosal resection (EMR) is difficult to apply (LSTnongranular [LST-NG] particularly the LST-NG, pseudodepressed type, lesions showing a VIŌĆÉtype pit pattern, carcinoma with shallow T1 [submucosa] invasion, large depressedŌĆÉtype tumors, and large protrudedŌĆÉtype lesions suspected to be carcinoma), mucosal tumors with submucosal fibrosis, sporadic localized tumors in chronic inflammatory conditions such as ulcerative colitis, and local residual or recurrent early carcinomas after endoscopic resection [8,9]. The European Society of Gastrointestinal Endoscopy also proposed that ESD can be considered for the removal of colonic and rectal lesions with a high suspicion of limited submucosal invasion, based on the 2 main criteria of depressed morphology and irregular or nongranular surface pattern (particularly if the lesions are >20 mm), or that ESD can be considered for colorectal lesions that otherwise cannot be optimally and radically removed using snare-based techniques [10]. All of the indications include tumors with superficial submucosal invasion as good candidates for colorectal ESD. Recently, an Australian group suggested that performing ESD only for lesions highly suspicious for containing submucosal invasive cancer is the most cost-effective strategy for removing large sessile tumors and LSTs >2 cm [11]. All the indications and studies suggest that estimation of the depth of invasion should be the priority when considering whether a colorectal neoplasm could be treated with endoscopic resection including ESD.
ESTIMATION OF INVASION DEPTH ACCORDING TO GROSS FEATURES
The depth of invasion can be estimated using the gross findings of white-light endoscopy. Size is one of the most important gross findings suggesting submucosal invasion. Submucosal invasion was found in 7.4%ŌĆō14% of colorectal polyps >2 cm in a Japanese study [12]. Other endoscopic features related to deep submucosal invasion were reported as follows: loss of lobulation, excavation, demarcated depressed area, stalk swelling, fullness, and fold convergence [13,14]. However, multivariate analysis revealed only loss of lobulation in the sessile type and fullness in the superficial type as the independent risk factors of deep submucosal invasion [13]. According to a Korean study including 39 superficial submucosal cancers and 25 deep submucosal cancers <2 cm, the positive predictive value and diagnostic accuracy for deep submucosal invasion of gross morphology assessment were 0.27 and 0.71, respectively, which are insufficient for clinical application [14]. The diagnostic accuracy of the 3 Korean experts who investigated the gross morphology were 74%ŌĆō82% for 15 submucosal cancers and 35 mucosal cancers, and their agreement was not high (╬║=0.298ŌĆō0.649) [15].
Although estimation of the invasion depth based on gross features may be simple, less resource consuming, and useful in selected cases, its diagnostic accuracy and interobserver agreement still seems insufficient for clinical application.
ESTIMATION OF INVASION DEPTH WITH NARROW-BAND IMAGING
Until 2009, several Japanese academic centers proposed their narrow-band Imaging (NBI) classifications (Sano, Hiroshima, Showa, and Jikei) based on the microvasculature pattern [16-19]. These classifications were used for histologic prediction and invasion depth estimation. Even a brief education on NBI magnifying endoscopy findings can improve traineesŌĆÖ accuracy in estimating the invasion depth [20]. However, there were concerns about the complicated classifications. In 2009, the Colon Tumor NBI Interest Group, which consisted of 6 experts from Japan, the United States, France, and the United Kingdom, proposed the NBI International Colorectal Endoscopic (NICE) classification. This classification is based on the color and the vascular and surface pattern of tumors, which can be assessed using nonmagnifying endoscopy. International studies have proved that this simple system is also useful for predicting the histology and estimating the invasion depth of colorectal lesions [15,21,22].
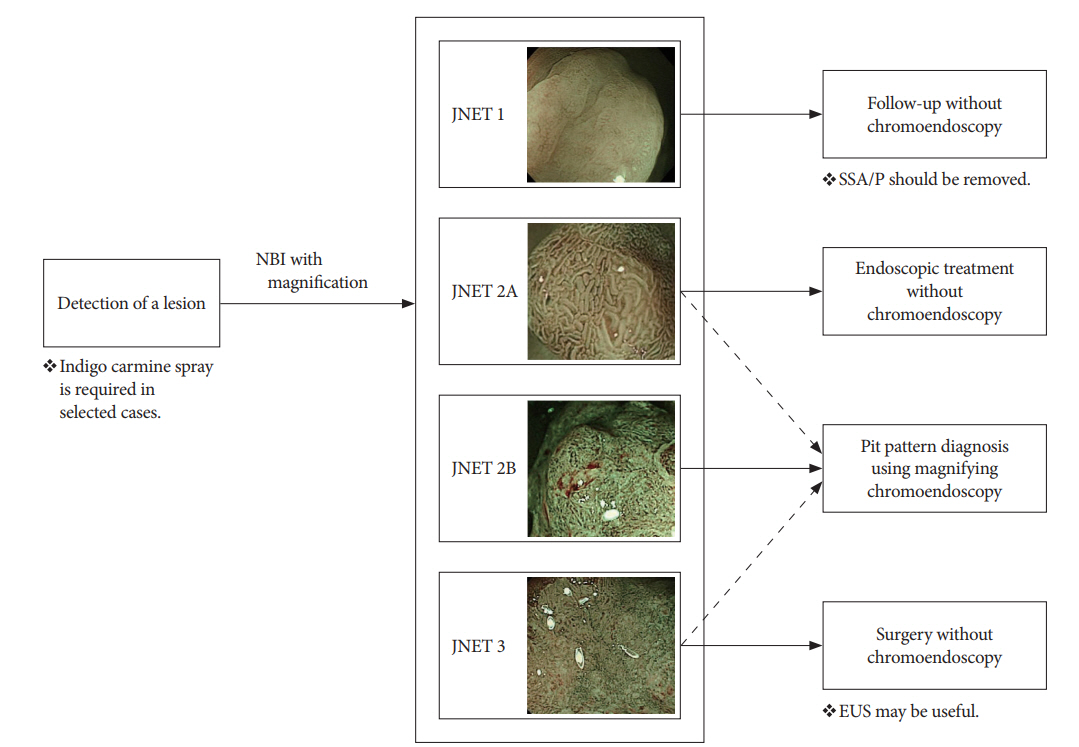
However, NBI findings suggesting superficial submucosal invasive cancer were not described in the NICE classification. In 2014, the Japan NBI Expert Team (JNET), comprising 38 Japanese specialists, proposed the JNET classification to unify the previous classifications of NBI magnifying endoscopy findings [23]. This classification was established to provide not only histologic prediction but also estimation of the invasion depth with NBI magnifying endoscopy [24,25]. This classification has 4 categories according to the vascular and surface pattern: JNET type 1, type 2A, type 2B, and type 3. Type 1 usually suggests hyperplastic polyp (HP) or sessile serrated polyp (SSP); type 2A is compatible with low-grade intramucosal neoplasms; type 2B includes high-grade intramucosal neoplasia or shallow submucosal invasive cancer; and type 3 means deep submucosal invasive cancer (Table 1) [23].
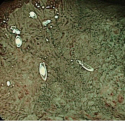
According to the Japanese studies that followed the JNET proposal, the classification was useful for the diagnosis of HP/SSP (type 1), low-grade dysplasia (type 2A), and deep submucosal cancer (type 3), but not for high-grade dysplasia/superficial submucosal cancer (type 2B). A retrospective image evaluation study revealed that the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy for type 2B lesions were 75.6%, 90.5%, 67.3%, 93.4%, and 87.4%, respectively [26]. Another study also showed that the specificity and positive predictive value of type 2B lesions judged by 3 expert endoscopists were 82.8% and 50.9%, which were lower than those of other type lesions [27]. Of lesions diagnosed as type 2B, 37% were low-grade adenomas and 12% were deep invasive cancers. Therefore, the authors proposed an additional evaluation, such as pit pattern diagnosis using chromoendoscopy, for the accurate diagnosis of type 2B lesions (Fig. 1) [27]. More data are required to evaluate how much the diagnostic accuracy for JNET type 2B lesions can be improved by additional magnifying chromoendoscopy.
ESTIMATION OF INVASION DEPTH WITH MAGNIFYING CHROMOENDOSCOPY
The surface of the lesion is washed with proteinase to remove overlying mucous for pit pattern diagnosis, after which indigo carmine solution is sprayed. When magnifying endoscopy with indigo carmine is not enough for an accurate pit pattern diagnosis, crystal violet solution is applied as a staining agent. However, the application of crystal violet may be limited outside of Japan because of the potential genotoxicity of this agent [28].
Studies on pit pattern diagnosis with magnifying chromoendoscopy have confirmed that specific categories of pit patterns are suggestive of submucosal invasive cancer. A study conducted at the Northern Yokohama Hospital showed that 34% of the lesions with a category VI (irregular) pit pattern and 91% of the lesions with a category VN (nonstructural/amorphous) pattern were submucosal cancers, whereas only 0.64% of pit pattern III or IV were submucosal cancers [12]. As mentioned above, the type VI pattern is associated with a variety of lesions, such as low-grade dysplasia, high-grade dysplasia/superficial submucosal cancer, and even deep submucosal cancer [29,30].
Therefore, there have been trials classifying the type VI pattern into subtypes for better prediction of invasion depth. Onishi et al. suggested that the following 4 patterns are suggestive of deep submucosal invasion: absence of pits that can be recognized as having originated from type III or IV, marginal irregularities of the gland duct, narrowing of the gland duct lumen, and unclear outline of the gland duct [29]. Matsuda et al. reported that the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy for 3,371 adenomas, 612 intramucosal cancers, 52 superficial submucosal cancers and 180 deep submucosal cancers were 85.6%, 99.4%, 86.5%, 99.4%, and 98.8%, respectively, when VI lesions with a demarcated area (clearly visualized zone between 2 morphologically different types of pits, e.g., depression, large nodule, or reddened area) were considered to have a deep submucosal invasive pattern [3]. Kanao et al. subclassified VI lesions into those with mild irregularity and those with severe irregularity (unclear staining between pits, irregular pit margins, and VI area Ōēź5 mm) [30]. They found that 56.1% of severely irregular lesions were deep submucosal invasive cancers, whereas 6.7% of mildly irregular lesions were deep submucosal invasive cancers [30].
ESTIMATION OF INVASION DEPTH WITH ENDOSCOPIC ULTRASONOGRAPHY
As insertion of an echoendoscope into the colonic lumen is not feasible, a high-frequency device (20-MHz miniprobe) is generally used to determine the depth of invasion. A hypoechoic area breaking into the third layer is usually considered to indicate deep submucosal invasion. As the penetration depth of a high-frequency probe is limited, it cannot be used for the evaluation of the invasion depth of a large sessile or pedunculated lesion.
The current data on the diagnostic accuracy of endoscopic ultrasonography (EUS) for estimating the invasion depth are conflicting. Two previous trials that were performed prospectively suggested that EUS was superior to magnifying chromoendoscopy, with a higher accuracy of invasion depth determination (92% vs. 63% [31] and 93% vs. 59% [32]). However, both studies had a limitation: when performing EUS, the endoscopists had more information because EUS was performed after magnifying chromoendoscopy. A recent prospective trial, with a cross-over design, on magnifying chromoendoscopy and EUS revealed that the diagnostic accuracy for depth of invasion was comparable between the two methods (71% vs. 71%); however, EUS required a significantly longer procedure time than magnifying chromoendoscopy, and the authors concluded that neither procedure has sufficient diagnostic accuracy [33].
ENDOCYTOSCOPY AND ARTIFICIAL INTELLIGENCE FOR INVASION DEPTH ESTIMATION
Ultra-high magnification images (├Ś450) can be obtained using an endocytoscope after staining with 0.05% crystal violet and 1.0 methylene blue, which stains cellular matrices and nuclei, respectively. In a pilot study, the diagnostic accuracy of endocytoscopy for deep invasive submucosal cancer was 95.9% [34]. Endocytoscopy images were also interpreted using artificial intelligence, and the algorithm obtained after 5,543 images from 238 lesions could diagnose invasive colorectal cancer in 200 test images with an accuracy of 94.1% [35].
PROPOSED STRATEGIES FOR COLORECTAL NEOPLASIA TREATMENT
Although noninvasive neoplasia can be resected using EMR or piecemeal EMR regardless of size, ESD can also be attempted for noninvasive lesions Ōēź2 cm, especially in experienced institutions, to accomplish en bloc resection and to decrease local recurrence. When a lesion with suspected superficial submucosal invasion cannot be optimally and radically removed using a snare-based technique, en bloc resection with ESD is strongly recommended. Surgical resection is definitely recommended for lesions for which there is high confidence about the presence of deep submucosal invasion [36].
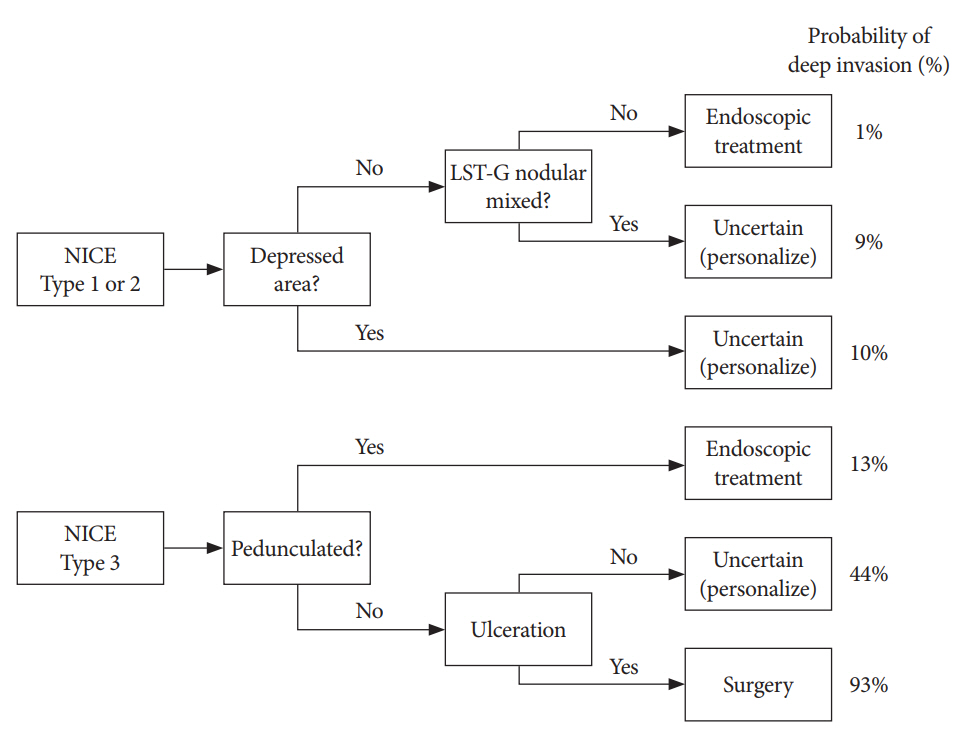
In a Spanish study analyzing 2,123 colon lesions >1 cm, a pedunculated morphology, ulceration, depressed area, or nodular mixed morphology affected the diagnostic accuracy of the NICE classification. Moreover, there remained subgroups of lesions for which endoscopic estimation of the invasion depth was difficult, including NICE type 2 with depressed area, NICE type 2 nodular mixed type, and NICE type 3 nonpedunculated polyps without ulceration. The authors proposed a management algorithm for polyps >1 cm according to the probability of deep invasion and endoscopic resectability (Fig. 2) [37].
Even with all the currently available modalities for estimating the invasion depth before colorectal ESD, including the assessment of gross features, NBI, and magnifying chromoendoscopy, a perfect estimation is not possible; thus, the clinical decision after colorectal ESD should be mainly based on the final histopathologic results. As mentioned earlier, additional surgery should be considered when the resected specimen shows unfavorable histologic findings [5,6].
CONCLUSIONS
Estimation of the invasion depth is an important step for successful colorectal ESD. Currently, NBI magnifying endoscopy is one of the most useful and practical methods of estimating the invasion depth of colorectal tumors. Although JNET type 2B (irregular vessel and surface pattern) represents high-grade intramucosal neoplasia/shallow submucosal invasive cancer, it also occasionally suggests deep submucosal invasive cancer or low-grade intramucosal neoplasm. Magnifying chromoendoscopy is recommended for JNET type 2B lesions, and more studies are required to elucidate how much diagnostic accuracy can be improved by additional magnifying chromoendoscopy.