INTRODUCTION
Peroral endoscopic myotomy (POEM) has been a minimally invasive treatment option for patients with achalasia for the past 10 years. Although comparable to laparoscopic HellerŌĆÖs myotomy (LHM) in terms of efficacy, POEM has the advantages of minimal invasiveness, allowance for a longer myotomy, and the ability to perform a posterior or anterior myotomy [1-6]. After 10 years of consistent safety and efficacy, POEM is now being performed worldwide and has been increasingly used in Latin America where Chagas disease is prevalent. Reports on POEM for Chagas disease are scarce [7-21]. POEM in Chagas disease is technically more challenging than in patients with achalasia, due to a higher rate of submucosal scarring [21], most likely related to chronic esophagitis caused by esophageal stasis (clinical observation, unpublished data). Two recently published studies have shown that Chagas disease-related achalasia responds better to POEM [15,22]. Nonetheless, the learning curve of gastroenterologists performing the procedure has not been well studied [16-21]. The aim of this study was to determine the learning curve for POEM among operators in Latin America.
PATIENTS AND METHODS
Consecutive patients diagnosed with achalasia who underwent POEM with a single operator in Argentina, Bolivia, Brazil, Colombia, Ecuador, Mexico, and Nicaragua between June 2013 and August 2017 were included in a prospective registry (ClinicalTrials.gov Identifier: NCT02162589). The single operator was previously proficient in endoscopic submucosal dissection (ESD). Informed consent for the procedure was obtained from all patients. Patient demographics, procedural information, post-procedural follow-up data, and adverse events were collected for all patients. Technical success was defined as successful completion of the myotomy. Clinical success was defined as an Eckardt score of Ōēż3 at 3 months.
Procedural technique
All procedures were performed under general anesthesia with endotracheal intubation. CO2 insufflation was used in all cases. A standard gastroscope fitted with a dissection cap was used. Initial upper endoscopy to clear the esophagus was performed, after which a mixture of saline solution and methylene blue was injected anteriorly or posteriorly. A longitudinal incision was made and a 12-cm longitudinal tunnel was created crossing the esophagogastric junction 2 cm into the stomach. The myotomy was performed in this tunnel. Ultimately, the mucosotomy was closed with endoscopic clips [9].
Clinical outcomes and statistical analysis
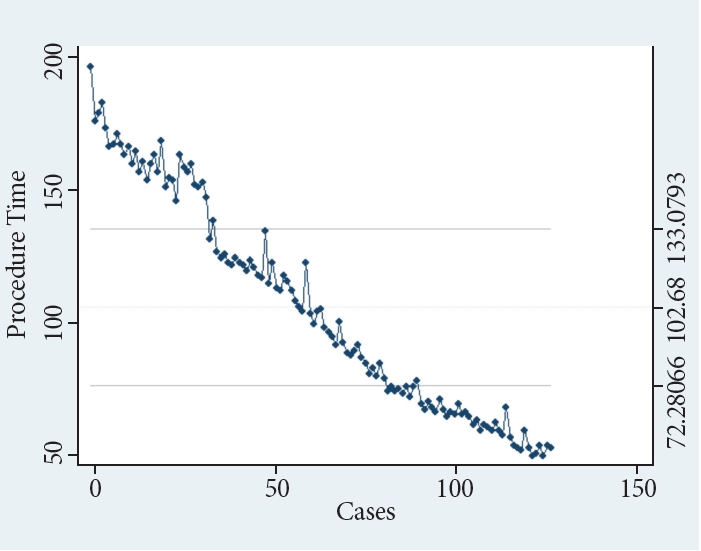
Demographics, clinical characteristics, pre- and post-procedure Eckardt scores, procedure duration, post-procedure follow-up data, and adverse events were collected. To measure the learning curve, non-linear regression was used with the case number as an independent variable and the procedure time as the dependent variable.
Cumulative sum control chart (CUSUM) analysis was conducted to report small shifts in procedure duration over time. The CUSUM analysis was performed similar to the modeling described by Biau DJ et al. [23]. Non-linear regression, CUSUM analyses test for independent means, and Fisher exact tests for proportions were conducted using Stata 15 (StataCorp LLC, College Station, TX, USA) . The primary outcome was the analysis of the learning curve, which was obtained by measuring the length of the procedure for consecutive procedures. The secondary outcomes were technical clinical efficacy based on the postoperative Eckardt score, adverse event rate, and reintervention rate.
RESULTS
Table 1 summarizes the main results of this study. A total of 125 patients were included (52% male; mean age, 59 years). The most common pathology was type II achalasia (n=80, 64%), followed by type I achalasia (n=9, 7.2%), type III achalasia (n=33, 26.4%), and other esophageal motility disorders (n=3, 2.4%). Chagas disease was present in approximately one-third of the patients (n=38, 30.4%). Most patients had undergone no prior treatment for achalasia (n=84, 67.2%). Previous treatments undergone by patients included prior LHM (n=18, 14.4%), pneumatic dilation (n=17, 13.6%), or botulinum toxin injections (n=6, 4.8%). The average pre-procedure Eckardt score was 6.79.
Technical success was achieved in 93.5% of patients (n=117). A total of 99 patients (79.2%) underwent posterior POEM, and 26 patients underwent anterior POEM (20.8%). The mean procedure duration in all cases was 97 min, ranging from 45 min to 196 min, with a mean of 102.7 min. There was no statistically significant difference (p=0.35) in the mean procedure duration of the Chagas group (mean =108 min; range, 48-196 min), when compared to that in the non-Chagas patients (mean=100.36 min; range, 46-175 min).
Mucosotomy entry was closed with standard endoclips in the majority of patients (n=120, 96%). Only in 5 cases (4%) were the mucosotomy closed with overstitch sutures.
Clinical success was achieved in 111 patients (88.8%). The mean post-procedure Eckardt score was 1.87. The clinical failure rate was higher in the Chagas group than in the non-Chagas group (21% vs. 7%, p=0.03).
On average, the median length of hospital stay was 1.98 days. The median follow-up period was 16 months (standard deviation [SD], 12.89 months).
Adverse events occurred in 27 patients (21.6%) and included mucosal perforation (n=13, 10.4%) closed during a second endoscopy by using clips, severe bleeding (n=4, 3.2%) solved using coagulation graspers and balloon tamponade, pneumothorax (n=4, 3.2%) requiring chest tube placement, leak (n=4, 3.2%) that resolved on repeat endoscopy and clip closure, and mediastinitis (n=2, 1.6%) managed with antibiotic therapy. The incidence of adverse events was higher in the Chagas group than that in the non-Chagas group (37% vs. 15%, p=0.01).
There was no statistically significant difference in reintervention rates between the Chagas group and the non-Chagas group (18% vs. 7%, p=0.06).
The CUSUM analysis (Fig. 1) revealed that the 97-minute procedure time was achieved at the 61st procedure, indicating efficiency. Aside from a few outliers, procedure duration further reduced with consequent procedures with the last 10 procedures under 50 minutes almost approaching a plateau (non-linear regression, p<0.01) (Fig. 2). We assume that further evaluation of the next 40-50 cases could potentially reveal a plateau, indicating mastery.
DISCUSSION
POEM has been well-established as a safe and efficacious procedure for the management of achalasia. In a meta-analysis of 36 studies that included 2,373 patients across 12 countries, 98% of patients with achalasia had clinical success (defined as a reduction in Eckardt score to Ōēż3) with POEM. The mean Eckardt score decreased from 6.9 ┬▒0.15 preoperatively to 1.0┬▒0.08 at 12 months postoperatively. In addition, there were significant decreases in the average lower esophageal sphincter pressure and the integrated relaxation pressure [24].
Previous studies have suggested that POEM in Chagas patients is technically more challenging due to significant amounts of submucosal scarring [15]. However, studies also suggest that patients with Chagas disease-related achalasia tend to respond better to POEM than to LHM [15].
Another recent study comparing POEM in Chagas vs. non-Chagas achalasia patients highlighted how the post-procedure Eckardt scores, procedure time, and repeat interventions differed between the groups. In the Chagas group, the post-procedure Eckardt score was reduced by 3.57 points compared to 6.03 in the non-Chagas group. Repeat intervention was much higher in the Chagas group than in the non-Chagas group (51% vs. 17%), and the mean POEM procedure time was longer in the Chagas group than in the non-Chagas group (120 minutes vs 94 minutes) [22].
In this study, we saw statistically significant higher adverse events and clinical failure rates in the Chagas group than in the non-Chagas group (37% vs. 15% and 21% vs. 7%, respectively).
There is limited published information on the learning curve of this procedure which includes achalasia patients due to Chagas disease. Kurian et al. looked at the learning curve of POEM and reported mastery of technique after 20 operations, demonstrated by decreased procedural time [11]. Patel et al. evaluated the experience of a single gastroenterologistŌĆÖs POEM learning curve in which they found that efficiency was achieved after 40 cases and mastery was reached after 60 operations [12]. Zein et al. analyzed multiple methodologies for assessing the learning curve and reported a learning rate of 13 cases and a ŌĆ£plateauŌĆØ at 102 minutes [13]. Liu et al. found that 100 cases were required to decrease the risk of technical failure, adverse events, and clinical failure, while 70 cases were the threshold for decreasing procedure time [9]. A recent study of 136 patients by Tefas et al. [25] reported a learning curve cut-off of 20 cases. They also noted that the major complication risk rate was higher during the learning curve (13.3%). However, the rate of minor complications was not influenced by operator competency during or after the learning curve cut-off.
Our study differs from the previous POEM learning curve studies as our analyses included Chagas patients, reflecting actual endoscopic experiences in the achalasia patient population in Latin America. Of the 125 patients included in the study, 30% had Chagas disease and the Chagas group had a higher incidence of adverse event rates than the non-Chagas group. There was no statistically significant difference in the procedure times between the groups, and the median procedure time was 97 minutes.
CUSUM analyses showed that a 97 minute procedure time was achieved at the 61st procedure and procedure duration progressively decreased, with the last 10 procedures performed in less than 50 minutes.
There are two limitations to this study. We did not compare multiple operators. Additionally, the expert endoscopist included in this study had prior proficiency in therapeutic endoscopy, including endoscopic submucosal dissection (ESD) and endoscopic mucosal resection (EMR). Thus, the learning curve might underestimate the number of therapeutic endoscopies and POEMs required to achieve POEM proficiency in endoscopists who lack such skills.
CONCLUSIONS
This Latin America learning curve study demonstrated that efficiency was reached at 97 minutes and at a learning rate of 61 cases, with continuing improvement. POEM seems to be a more technically difficult procedure to master in Latin America, requiring a higher volume of cases to reach efficiency, and also seems to be associated with a higher number of adverse events in the initial phase of the learning curve. Most likely, these obstacles are related to the increased anatomical challenges observed in patients with Chagas disease. We recommend that only endoscopists demonstrating proficiency in ESD and EMR should conduct POEM procedures.