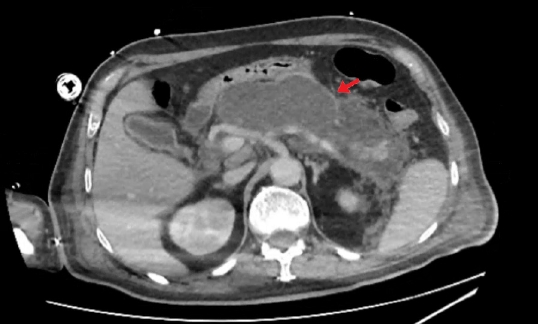
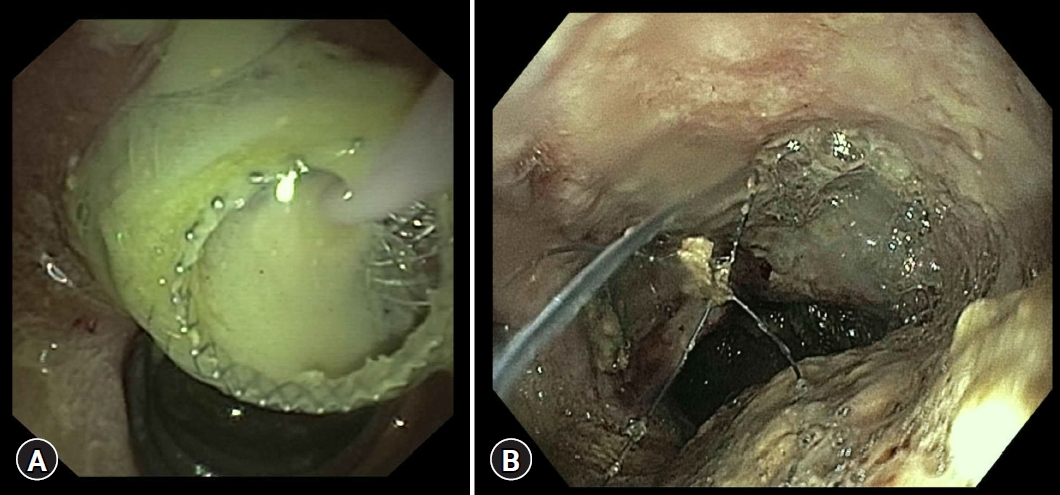
Endoscopic ultrasound (EUS)-guided transluminal drainage through deployment of a lumen-apposing metal stent (LAMS) is a safe and effective technique for pancreatic fluid collections,1,2 even without fluoroscopy.3 The LAMS placement has changed the approach to various diseases, simplifying drainage and necrosectomy techniques to a point that difficult necrosectomies consider the removal and replacement of the same LAMS.4 The removal of LAMS is usually technically safe, and the use of different devices (snare and forceps) can be easily achieved through the gastrointestinal tract. Herein, we present the case of a 67-year-old man with severe acute pancreatitis who developed a huge walled-off pancreatic necrosis (WOPN), which became symptomatic (nausea, vomiting, and gastric outlet obstruction) and infected. Computed tomography scan revealed an 18-cm WOPN (Fig. 1). Therefore, the patient was referred to our institute for EUS-guided drainage. WOPN drainage was achieved with deployment of a LAMS 20У10 mm, with the generation of a gastrocystostomy utilizing the тfree-handт technique with a Hot Axios device (Boston Scientific, Marlborough, MA, USA), followed by endoscopic necrosectomy with partial cleansing of the cavity (Fig. 2). At that point, the patient was critically ill and developed multiorgan failure and septic shock; therefore, he was admitted to the intensive care unit. A computed tomography scan revealed unmodified WOPN. The patient was treated using the multiple transluminal gateway technique, deploying a second LAMS in the duodenum (10У15 mm). Other necrosectomies were performed until complete cleansing of the cavity was achieved and the patient recovered clinically. We then proceeded to remove the distal (duodenal) LAMS three weeks after its placement, but the classical LAMS removal through the duodenum seemed uncomfortable and unsafe. Therefore, it was directly removed from the collection cavity through the proximal (gastric) LAMS, which was also removed after five weeks of indwelling (Supplementary Video 1). Specifically, we decided to remove the distal LAMS with an alternative way for duodenal wall- and technique-related reasons. On one hand, we included the duodenal LAMS location (posterior wall of the duodenal bulb, on the corner between the first and second duodenum), which did not permit a proper grab of the flange, and the severe inflammation of the duodenal mucosa and thinness of the wall contributed to considering the duodenal wall to be too fragile to perform an extreme torsion of the scope with the devices over it. On the other hand, we had a large space and lack of vessels in the cavity, and a larger diameter of the gastric LAMS (20 mm) compared to the duodenal LAMS (15 mm). In the end, the association of the above-mentioned reasons led us to consider trans-duodenal removal to be dangerous, while the trans-LAMS removal was considered safe. In the final analysis, the patient fully recovered without complains of technique-related adverse events. He was discharged after two weeks. In conclusion, WOPN treatment with a multi-gate approach is an effective and safe endoscopic technique when the WOPN is >12 cm.5 In cases of risky trans-duodenal removal, the duodenal LAMS inner removal through the gastric LAMS is a feasible and safe alternative option in patients treated with a multi-gate approach.