INTRODUCTION
Inflammatory bowel disease (IBD), including CrohnÔÇÖs disease (CD) and ulcerative colitis (UC) is associated with an increased risk of colorectal cancer (CRC), especially in patients with extensive inflammation and longer disease duration without remission.1,2 Frequent screening colonoscopy and surveillance of colorectal dysplasia in patients with IBD have demonstrated a decreased risk of advanced and interval CRC. However, this entirely depends on identifying and effectively resecting the colorectal dysplasia.3
Endoscopic removal of dysplastic lesions by endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) in IBD can be challenging because of chronic inflammation and extensive submucosal fibrosis. In the past, dysplasia in IBD was managed by surgical resection; however, the emergence of endoscopic resection has reduced the need for surgical intervention.4 Current guidelines recommend surgery to be reserved for endoscopically unresectable and invisible high-grade dysplasia in IBD. The American Society of Gastrointestinal Endoscopy (ASGE) guidelines and the Surveillance for Colorectal Endoscopic Neoplasia Detection and Management in Inflammatory Bowel Disease recommend endoscopic resection of visible dysplastic lesions with distinct borders and absence of submucosal invasion.5,6
EMR may not be effective for large dysplastic lesions (>2 cm), especially with the presence of submucosal invasion or friable mucosa.4,7,8 The ESD technique overcomes the limitations of EMR for dysplastic lesions in IBD by allowing en-bloc resection of lesions, regardless of size and presence of submucosal fibrosis.9-11 It facilitates detailed histological examination of the resected lesion and significantly reduces the risk of recurrence.4,8 Evidence regarding the outcomes of ESD for colorectal dysplasia in IBD is limited to smaller retrospective, single-center studies. We conducted this meta-analysis to appraise the current literature regarding the safety and efficacy of ESD for colorectal dysplasia in IBD.
METHODS
Search strategy
Multiple databases, including PubMed, Scopus, Embase, and Cochrane, were comprehensively searched from their inception until October 2022. The search was limited to studies in the English language only, and animal studies were excluded. The search strategy was designed and conducted by an experienced librarian with input from the studyÔÇÖs principal investigator. Keywords and controlled vocabulary were used to search for studies on ESD in patients with IBD. The full literature search strategy is provided in Supplementary Material 1. Reference lists of articles were analyzed to identify studies missed on the initial search. Preferred reporting items in meta-analysis,12 and meta-analysis of observational studies checklists were followed,13 and are summarized in Supplementary Materials 2 and 3.
Study selection
Studies reporting outcomes of ESD for colorectal dysplasia in patients with IBD; comprising UC, CD, or both UC and CD; and with appropriate data including resection and adverse event rate regardless of study setting, geographical location, or follow-up period were included.
Studies were excluded based on the following criteria: (1) involving animal subjects, (2) involving patients aged <18 years, (3) not published in the English language, (4) involving hybrid ESD, (5) with a sample size of less than five, and (6) not published as full manuscripts (abstract or conference proceedings). Two reviewers carefully reviewed each study for eligibility based on the above-mentioned criteria. The authors were contacted by e-mail for any clarifications regarding study data.
Data extraction
Data extraction was performed by two reviewers (TFM and VS), and a third author analyzed the data (BPM). Data regarding study and patient characteristics and outcomes were extracted onto a standardized form. In case of any discrepancy, a consensus was achieved by discussion with the senior author (GSK). Authors of the included studies were contacted by e-mail if further information on study data was needed.
Outcome assessment
We assessed the following outcomes: pooled rates of en-bloc resection, R0 resection, curative resection, adverse events (bleeding and perforation), local and metachronous recurrence, and additional surgery after ESD. Based on data availability and feasibility, predetermined subgroup analyses were planned based on the IBD type (UC, CD, and UC+CD), study sample size (<20 or >20), and geography (United States [US], Asia, and others). Meta-regression was planned based on lesion location (right or left), morphology (polypoid or nonpolypoid), lesion border (distinct or indistinct), and surrounding mucosa (remission or active) to assess potential causes of heterogeneity and predictors of clinical outcomes.
1) Assessment of methodology and definitions
The quality of each study was assessed using the Newcastle-Ottawa scale for cohort studies.14 Two authors assessed and scored each study independently (TFM and VS). Details of the individual study scoring are provided in Supplementary Table 1.
Data on resection, recurrence, and adverse event rates were collected from the original studies. En-bloc resection was defined as the complete removal of the lesion in one piece. The pooled rate of R0 resection was defined as the complete removal of the lesion with negative histological margins. Variability was observed with the definition of ÔÇÿcurative resection.ÔÇÖ The most consistent definition for ÔÇÿcurative resectionÔÇÖ was when pathological findings revealed R0 resection without any of the following features: submucosal deep invasion (ÔëÑ1,000 ╬╝m), lymphovascular involvement, or poorly differentiated adenocarcinoma component. Bleeding and perforation events, as reported in the original studies, were considered adverse events. Local recurrence was defined as the presence of dysplastic lesion at the resection site during follow-up colonoscopy. Metachronous tumor was defined as a new lesion detected in a colorectal area, other than the primary lesion site, more than six months following ESD.
Statistical analysis
We used meta-analysis techniques, particularly the random-effects model, to calculate the pooled estimates in each case following the methods suggested by DerSimonian and Laird. When the incidence of an outcome was zero in a study, a continuity correction of 0.01 was added to the number of incident cases before statistical analysis. Pooled proportions with corresponding 95% confidence intervals (CIs) were calculated for categorical outcomes, and pooled mean differences were calculated for continuous outcomes. We assessed heterogeneity between study-specific estimates using the Cochran Q statistical test for heterogeneity; 95% prediction interval (PI), which deals with the dispersion of the effects; and I2 statistics. We considered values of <30%, 30% to 60%, 61% to 75%, and >75% to indicate low, moderate, substantial, and considerable heterogeneity, respectively. Publication bias was ascertained qualitatively via visual inspection of the funnel plot and quantitatively using the Egger test. All analyses were performed using the Comprehensive Meta-Analysis (CMA) software ver. 4 (BioStat).
RESULTS
Search results and population characteristics
The initial search generated 103 studies, of which 47 duplicates were removed and 56 studies were screened and fully assessed. Twelve studies were included in the final analysis.15-26 The schematic flow diagram for the study selection process is illustrated in Supplementary Figure 1.
A total of 291 dysplastic lesions were removed by ESD in 274 patients. The median age was 62 years (interquartile range, 54ÔÇô65). Of the patients, 56% were male (n=167), and 44% were female (n=132). The mean lesion size was 28.6 (18.25ÔÇô40.7) mm. Approximately 77.3% of lesions were in the left colon (n=184), 80.7% were nonpolypoid (n=192), and 73.2% had submucosal fibrosis (n=161). The overall mean procedure time was 72.7 (95% CI, 53.2ÔÇô92.2) minutes (Supplementary Fig. 2). The median study follow-up time was 25 months. Further study and baseline patient characteristics and study outcomes are summarized in Tables 1 and 2, respectively.15-26
Characteristics and quality of included studies
Three studies were prospectively conducted,15,17,21 and five studies were multicenter studies.15,18,21,23,25 The assessment of study quality is detailed in Supplementary Table 1. Overall, two studies were considered high quality, and ten studies were medium quality. No low-quality studies were identified.
Meta-analysis outcomes
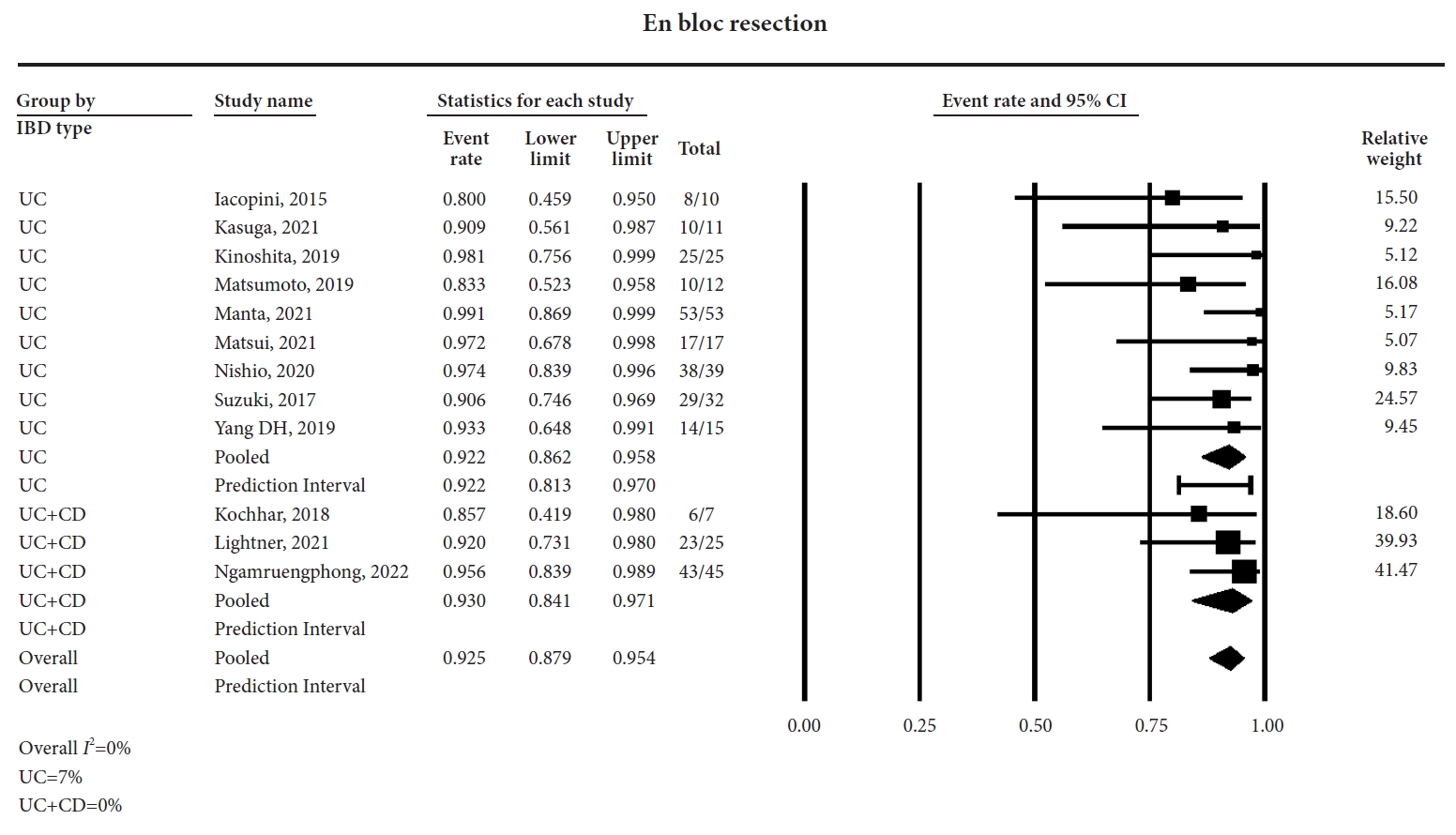
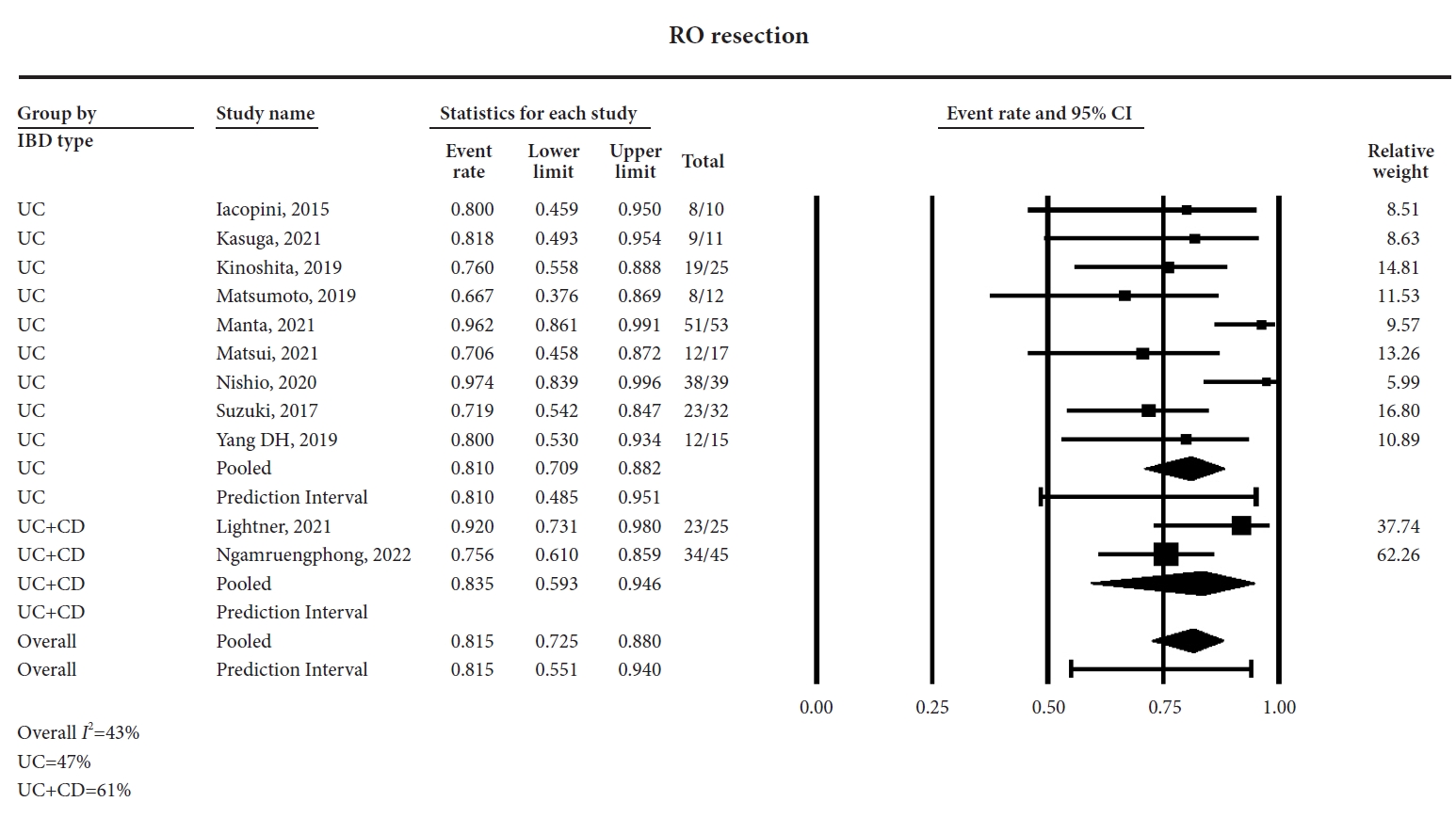
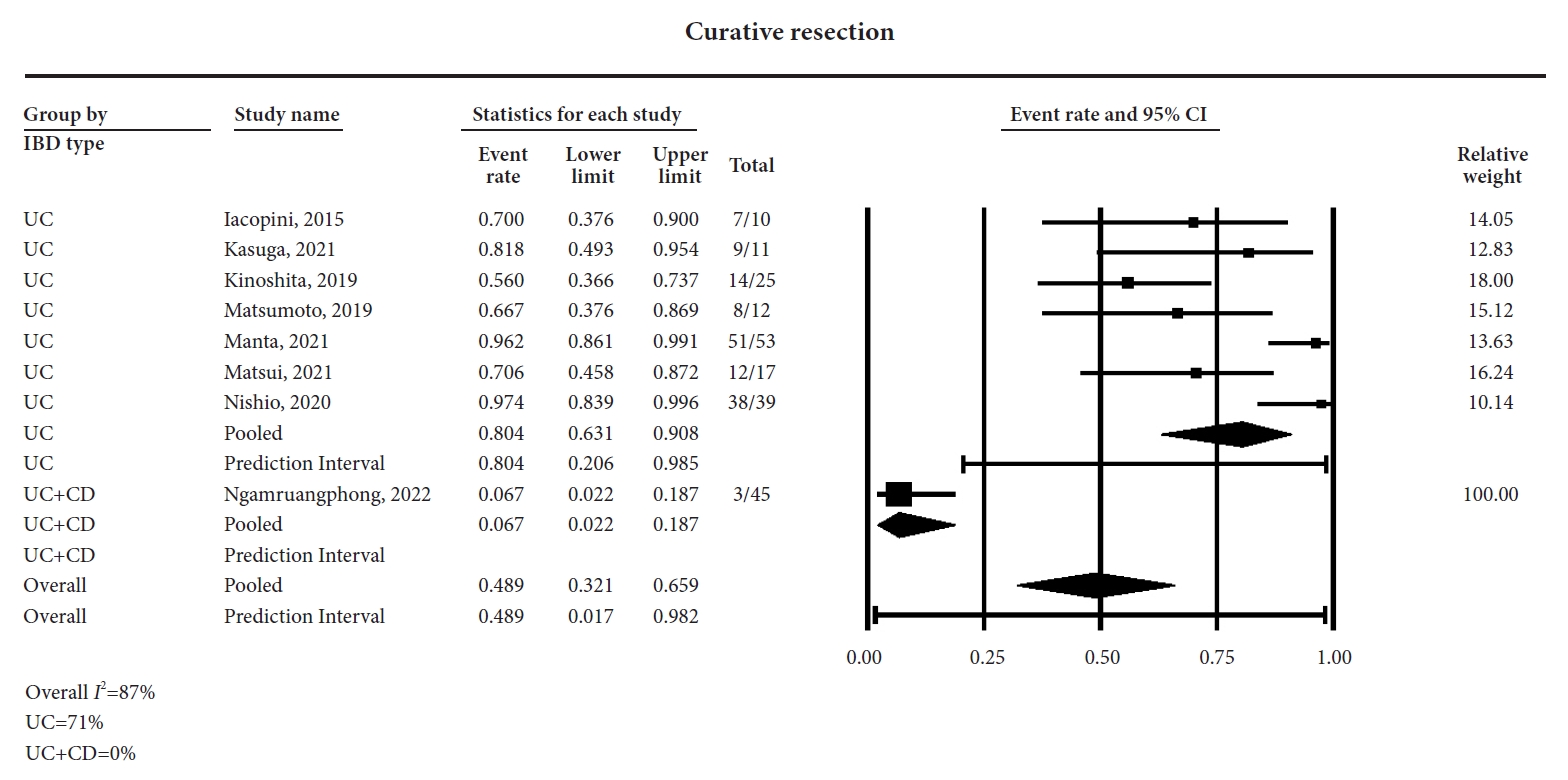
ESD was performed for a total of 291 dysplastic lesions in 274 patients with IBD. The pooled rates of en-bloc, R0, and curative resections were 92.5% (95% CI, 87.9%ÔÇô95.4%; I2=0%) (forest plot, Fig. 1), 81.5% (95% CI, 72.5%ÔÇô88%; I2=43%) (Forest plot, Fig. 2), and 48.9% (95% CI, 32.1%ÔÇô65.9%; I2=87%) (forest plot, Fig. 3), respectively. The local recurrence and metachronous recurrence rates were 3.9% (95% CI, 2%ÔÇô7.5%; I2=0%) (forest plot, Supplementary Fig. 3) and 10% (95% CI, 5.2%ÔÇô18.2%; I2=55%) (forest plot, Supplementary Fig. 4), respectively.
The rate of additional surgery following ESD was 13% (95% CI, 8.5%ÔÇô19.3%; I2=54%) (forest plot, Supplementary Fig. 5). The causes for requiring additional surgery after ESD included presence of superficial or submucosal tumor invasion, lymphatic and vascular involvement, metachronous lesions, invasive adenocarcinoma, and medically refractory disease. One patient with severe submucosal fibrosis received surgery after unsuccessful ESD.
The pooled rates of bleeding and perforation were 7.7% (95% CI, 4.5%ÔÇô13%; I2=10%) (forest plot, Supplementary Fig. 6) and 5.3% (95% CI, 3.1%ÔÇô8.9%; I2=0%) (forest plot, Supplementary Fig. 7), respectively. When perforation occurred during ESD, it was treated endoscopically using clip placement and did not require surgery. The pooled rates and I2% values are summarized in Table 3.
Subgroup and meta-regression analysis
1) Subgroup analysis based on IBD type (UC only and UC+CD)
In nine studies, ESD for colorectal dysplasia was performed in patients with UC only. Three studies have reported on ESD for colorectal dysplasia in both UC and CD. The en-bloc resection rates were 92.2% (95% CI, 86.2%ÔÇô95.8%) in studies with UC and 93% (95% CI, 84.1%ÔÇô97.1%) in studies with UC+CD. The R0 resection rates were 81% (95% CI, 70.9%ÔÇô88.2%) for UC and 83.5% (95% CI, 59.3%ÔÇô94.6%) for UC+CD. The rest of the subgroup analyses were limited owing to fewer studies on the UC+CD group. The results are summarized in Table 3.
2) Subgroup analysis based on sample size (<20 or >20) and study geography
Six studies had a sample size of <20 patients. Equally, six studies had a sample size of >20 patients. Three, six, and three studies were conducted within the US, Asia, and outside the US and Asia (Italy and United Kingdom), respectively. The subgroup analysis based on study sample size and geography was primarily performed for sensitivity analysis to ascertain potential contribution toward the observed heterogeneity. The outcomes were comparable in studies performed in the US, Asia, and other regions. The results are summarized in Supplementary Table 2.
A meta-regression analysis was performed based on lesion location (right or left), morphology (polypoid or nonpolypoid), lesion borders (distinct or indistinct), and surrounding mucosa (remission or active). However, statistical analysis was not feasible due to the limited number of studies.
Validation of meta-analysis results
1) Sensitivity analysis
To assess whether any study had a dominant effect on the meta-analysis outcomes, we excluded one study at a time and analyzed its effects on the main summary estimate. In this analysis, no single study significantly affected the outcome or heterogeneity.
2) Heterogeneity
No heterogeneity was noted for the primary outcomes of en-bloc resection, whereas moderate heterogeneity was observed for R0 resection. Overall, heterogeneity was moderate except for curative resection (87%). This was most likely attributable to the lack of a uniform definition for curative resection among the studies. The subgroup analysis demonstrated sample size (<20 vs >20) as a significant contributor toward the pooled local recurrence. Since the random-effects model was used, the 95% PIs are illustrated in the respective forest plots.
3) Publication bias
No publication bias was noted based on the qualitative assessment of the funnel plot (Supplementary Fig. 8) and quantitatively by EggerÔÇÖs regression analysis (two-tailed p-value = 0.06).
4) Quality of evidence
The GRADE working group approach was used to rate the quality of evidence for results from this meta-analysis.27 Based on the retrospective nature of included studies and moderate heterogeneity, this meta-analysis would be considered to have low-quality of evidence.
DISCUSSION
In this meta-analysis of twelve studies, ESD demonstrated an excellent pooled en-bloc (92.5%) and R0 (81.5%) resection rate for colorectal dysplasia in patients with IBD. The local recurrence rate was 3.9%, with low pooled rates of adverse events, including bleeding (7.7%) and perforation (5.3%). To the best of our knowledge, with 291 dysplastic lesions in 274 patients with IBD, this study reports the largest pooled data of ESD for colorectal dysplasia in patients with IBD.
The current ASGE guidelines regarding the management of colorectal dysplasia in IBD recommend en-bloc resection by EMR or ESD of endoscopically visible lesions with distinct borders instead of surgery.8 EMR has been associated with a 27%ÔÇô63% en-bloc resection rate and a 14%ÔÇô50% local recurrence rate.11,28,29 In this study, although 73.1% of dysplastic lesions had submucosal fibrosis, ESD demonstrated excellent en-bloc and R0 resection rates along with low rates of local recurrence, perforation, and bleeding.
ESD in patients with IBD can present technical challenges if the submucosal fibrosis is extensive. This is reflected in our study with a metachronous recurrence rate of 20%. Despite this, we demonstrate that the need for surgery was low at 13%, with a curative resection rate of 48.9%. This may be attributed to not all patients with failed resection receiving surgery. Additionally, the rate of curative resection needs to be interpreted with caution as a certain level of variability was observed in how the individual studies defined ÔÇÿcurative resection,ÔÇÖ which also explains the high heterogeneity (87%). The most consistent definition for ÔÇÿcurative resectionÔÇÖ was when pathological findings revealed R0 resection without any of the following features: submucosal deep invasion (ÔëÑ1000 ╬╝m), lymphovascular involvement, or poorly differentiated adenocarcinoma component. The reported pooled rates are encouraging and highlight the importance of frequent endoscopic surveillance following ESD to monitor for local and metachronous recurrence in patients with IBD.
EMR is increasingly being performed in the US, whereas ESD remains a complex procedure only performed by experienced endoscopists in select IBD centers.30 In our analysis, the pooled mean procedure time was 72.7 minutes, which is comparable to the mean procedure time in ESD for sporadic CRC (75ÔÇô106 minutes).31,32 As the current literature demonstrates the increasing feasibility of ESD for complex lesions in IBD, we anticipate increased utilization of this technique with additional focused training.
In our subgroup analyses, we observed that pooled rates from studies with a sample size of >20 patients demonstrated lower rates of local recurrence (2% vs 7.3%). Although no studies that were exclusively performed in patients with CD were identified, we noted that the outcomes were slightly better in study samples that included both CD and UC compared to UC alone. Whether this is directly related to the differences in the underlying pathology of CD vs. UC or to the higher risk of dysplastic lesions in UC with varying grades of active inflammation contributing to indistinct lesion borders remains unknown.
A meta-analysis by Mohapatra et al. summarized the results of 190 colorectal dysplastic lesions undergoing ESD and revealed an en-bloc resection rate of 85.7% in patients with IBD.33 Similarly, a meta-analysis by Chen et al. demonstrated an en-bloc resection rate of 86% with ESD for non-polypoid dysplasia in patients with IBD.34 Our study demonstrated a higher en-bloc resection rate (92.5%) than the previous studies which may be attributed to the larger sample size with more recent studies included in our analysis. Recent advances in ESD techniques and emphasis on advanced training may have contributed to these findings.
Our study has several strengths. The literature search was rigorously performed to include studies that used ESD for colorectal dysplasia in IBD. No low-quality studies were identified in this analysis, and no heterogeneity was reported on the primary outcomes of en-bloc and R0 resection. As noted above, although studies reporting outcomes of advanced endoscopic resection techniques for colorectal dysplasia exist, the present study is the most up-to-date meta-analysis specifically evaluating outcomes of ESD technique for colorectal dysplasia in IBD.
This study had some limitations, most of which are inherent to any meta-analysis of retrospective studies with a potential risk of selection bias. Patient-level granular information regarding the severity of disease, extent of disease, and endoscopic remission status at the time of ESD was not available. Furthermore, information regarding the criteria of lesion selection, degree of dysplasia, timing of bleeding (immediate/delayed), and outcomes of patients who did not receive additional surgery after ESD could not be ascertained from all the studies. Additionally, concomitant high-risk features, such as positive family history, prior personal history of high-risk dysplasia, and primary sclerosing cholangitis, were not reported. Nevertheless, the pooled data from this study adds valuable information to the current literature on this topic.
In conclusion, this meta-analysis demonstrates ESD to be safe and effective for colorectal dysplasia in IBD. ESD demonstrates excellent en-bloc and R0 resection rate, with low rates of local recurrence and adverse events. The reported rates of curative resection warrant further studies with uniform definition to validate our findings.